Search
These authors argue that bystander interventions in the early minutes (they call them the diamond minutes) can have an impact on trauma survival. Particular attention to External hemorrhage control; Airway opening and maintenance; Safe positioning of unconscious patients; Mitigation of early hypoxia and hypothermia could improve survival. We need to publicize this information and undo the years of teaching not to move these patients due to concern of secondary spinal cord injury. Many studies have dispelled that concern.

Show References
This article suggest that freeze-dried plasma (FDP) is an acceptable adjunct to whole blood for prehospital resuscitation of trauma patients. “FDP is pathogen-reduced, shelf-stable for up to two years at room temperature, lightweight, and rapidly reconstituted at the point of care.” This method offers an advantage when caring for patients in remote areas with long transport times and has been used by NATO and Canadian armed forces.
Show References
Of the 215 Norwegian patients on oral anticoagulation seen for a head injury and having a normal initial head CT, none developed delayed hemorrhage. Median age was 83 years.
Show References
A recently published commentary highlights the importance of looking beyond the numbers and remembering the core mission of emergency practice. It warns against “gaming” the system to create processes that give better metrics using the example of rates of patients who leave without being seen (LWBS). In the author’s words, efforts aimed at improving this metric create strategies that “raise concerns about distributive justice, beneficence, and professional integrity.” See link for key take home points.
Show Additional Information
Show References
Sodium bicarbonate significantly reduced the need of renal replacement therapy (risk ratio [RR] 0.69; 95% CI, 0.61–0.78) but not mortality (RR, 0.84; 95% CI, 0.55–1.30). However, there was not enough sample size to support the outcome of mortality.
There was still significant heterogeneity between studies as the sources of metabolic acidosis were different between different studies in this meta-analysis study of randomized control trial. One study recruited patients with septic shock only, while other studies enrolled patients with different disease states.
There was also heterogeneity in the threshold for pH to enter the study.
Show References
Bottom Line: In adults presenting to the ED with bacteremia, bandemia may be associated with increased short-term mortality, with higher band percentages correlating with greater risk. Although bacteremia is rarely diagnosed during the ED visit because blood cultures require time to result, the presence of bandemia should raise concern for possible occult critical illness.
Show Additional Information
Show References
20yo college swimmer presents to the ED with a constellation of non-specific symptoms such as poor sleep, fatigue, depression/anxiety, weight loss.
Despite regular 2/day practices, his coach tells him his performance is worse than ever.
Show Additional Information
Previous pediatric studies have shown that 1) air transport has shown improved outcomes compared to matched ground transports but 2) air transport may be overutilized.
This was a multicenter retrospective study using the Pediatric Emergency Care Applied Research Network Registry from 2012-2021 looking at pediatric patients transported to the ED by helicopter. This registry does not differentiate between field transports and interfacility transfers. The study looked to identify patients who were discharged from the ED or had a hospital stay < 48 hours. 7722 patients were included with a median age of 5.9 years. 20% of these patients were discharged from the ED. Among those admitted, over half were discharged within 48 hours. Patients who were discharged from the ED were found to have triage < ESI 1, missing a systolic blood pressure or temperature. Tachycardia, tachypnea, hypertension and abnormal temperature were associated with a lower rate of ED discharge.
Bottom line: Additional research is needed to identify patients who may be more appropriate for ground transport or when transport is not needed (or could be replaced with telemedicine).
Show References
Not all patients with an acute PE will be crashing and critically ill, but it seemed worthwhile to remind everyone that there are new guidelines and recommendations from AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN/XYZLMNOP about the management of patients with acute pulmonary embolism in the 2026 AHA/ACC Joint Committee statement. A few key takeaways, with highlights for the sicker PE patients:
- New Classifications A through E for acute PE (see images below)
- Get familiar with the clinical scores! Hestia, PE Severity Index (PESI), simplified PESI (sPESI)
- ED discharge recommended for Category A and supported for Category B
- LMWH recommended over unfractionated heparin when parenteral AC is needed, unless contraindicated
- DOACs recommended over warfarin unless contraindicated
Highlights for the sicker PE patients, i.e. Categories C+:
- Get a look at the RV! (POCUS, CT, formal echo)
- Further stratify Category C patients/identify Category D earlier
- Find out how close to decompensation the patient might be
- Inform your management if the patient decompensates
- For PE patients with e/o RV strain (C2+ per this document; for me, particularly those C3+ with respiratory complaints as a marker of poor pulmonary perfusion, or Category D+), consider use of inhaled vasodilators
- Be careful with any sedation even if normotensive – decreasing preload / blunting the body's compensatory adrenergic response can be disastrous, have hemodynamic support available
- If you have to intubate, choose induction meds wisely and have hemodynamic support ready
- For patients with Category D-E acute PE:
- Norepinephrine = initial vasopressor of choice for hypotension due to modest inotropic effects; max at 15mcg/min due to effects on pulmonary vascular resistance at higher doses, if second vasopressor needed, reach for vasopressin
- Dobutamine as additional inotropic support OR for normotensive shock
- Avoid fluid boluses unless patient is also hypovolemic, and then give small boluses (250mL) only
- Consider advanced therapies for Category D and particularly E
- PE Response Team (PERT) Consultation recommended – and depending on where you practice, can help get the patient transferred if advanced therapies are an option
For a great breakdown and further discussion of the new guidelines, I recommend checking out the Life in the Fast Lane blogpost here.


Show References
This is a small qualitative study that focused on barriers to care and how to overcome them when dealing with patients with dementia, who are primarily Spanish speaking. The authors found to big themes that patients and caretakers thought would improve their care:
1- use of a certified translator, either telephonically or in person, eased social dynamics in communication
2- those same translators tended to only be used in an episodic manner- during HPI, exlaining results or discharge planning. But the patients and caretakers would prefer to have access to them in the “in between” periods so that it would be a more patient centered experience
Show Additional Information
Here are two techniques to remove a helmet from an injured motorcyclist. The first uses a cast saw to bivalve the helmet. A link for a video is also provided.
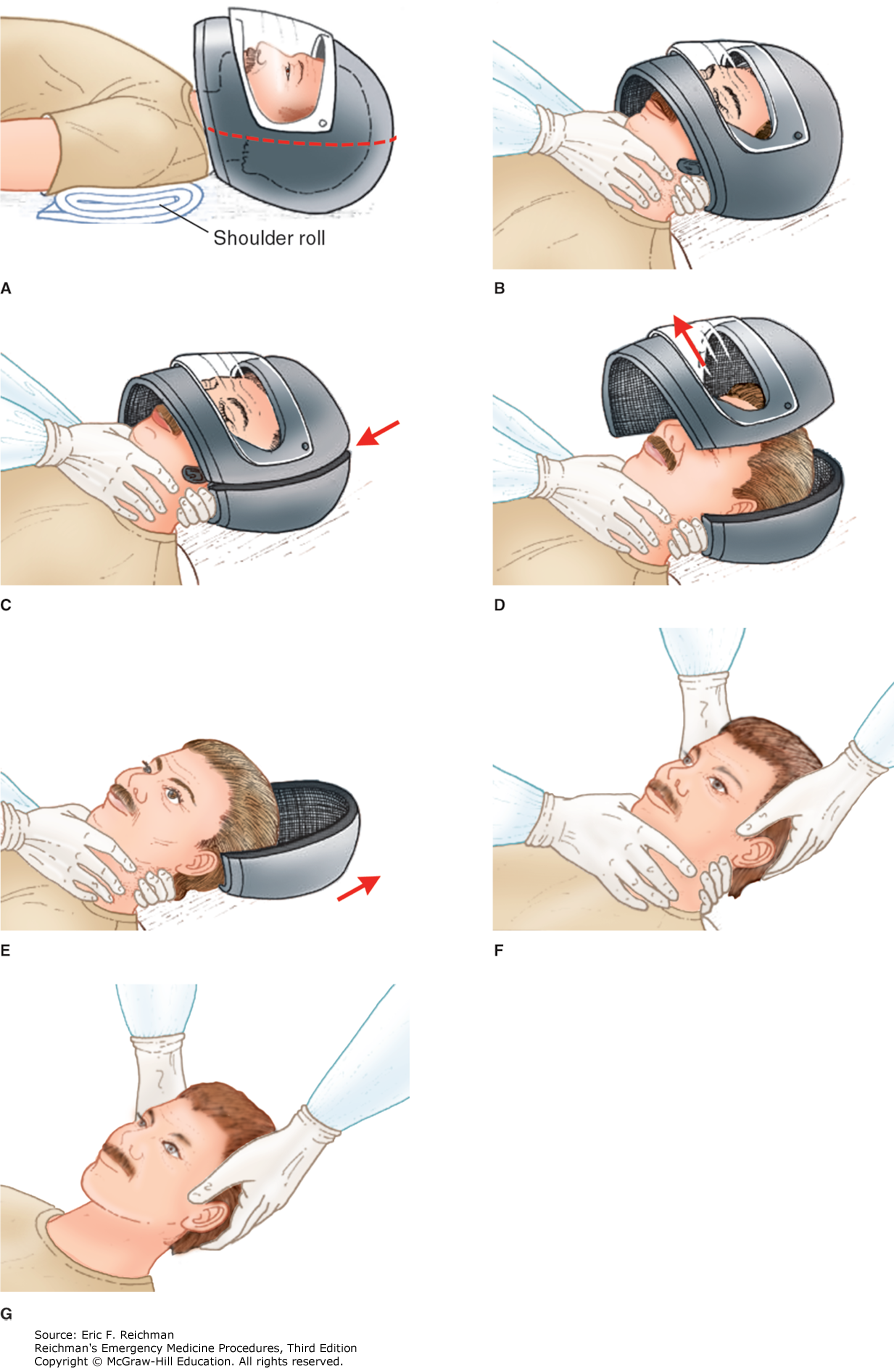
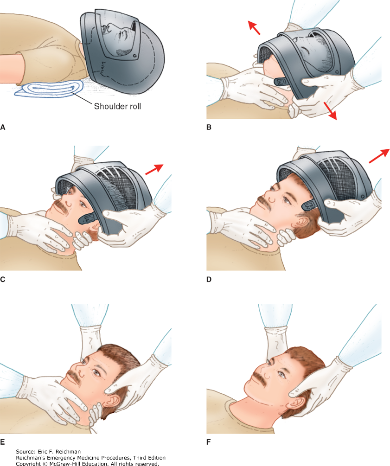
Show Additional Information
Show References
US and International guidelines differ on the initial defibrillation dose in pediatric patients. International, European, Australian and New Zealand guidelines had recommend an initial dose of 4 J/kg for the initial and all subsequent doses while the American Heart Association recommends an initial dose of 2-4J/kg (with 2 J/kg in the teaching algorithms) with subsequent shocks being at least at 4J/kg and no greater than 10 J/kg. More recently, ILCOR suggested an initial dose of 2-4 J/kg.
This was a systemic review of 7 observational studies, mostly involving in hospital pediatric cardiac arrests. Outcomes of termination of VF/pVT, ROSC and survival to hospital discharged were examined in relation to the initial J/kg dose that was used compared to initial doses of 2 J/kg. Outcomes were neither better or worse with doses < 1.5 J/kg or > 2.5 J/kg. Additional research is needed as this certainty of this evidence was considered “very low.”
Show References
Access to reproductive care is being limited across the country, and the rate of undesired pregnancies is rising.
Discussing contraception preferences in the Emergency Department can support patients as well as and reduce the morbidity and mortality associated with an undesired pregnancy. Simply asking patients of childbearing age: "Are you interested in discussing pregnancy prevention?" can bridge a gap in access to reliable care. Easy and accessible tools can be used on shift to assist with appropriate initiation.
On Shift Tools:
Contraception Initiation • Clinical Resources • FemInEM
www.bedsider.org -Patient friendly comparisons of contraception options
Quick Start Contraception Care in the ED - Bridge to Treatment - ED oriented flow diagram
Show References
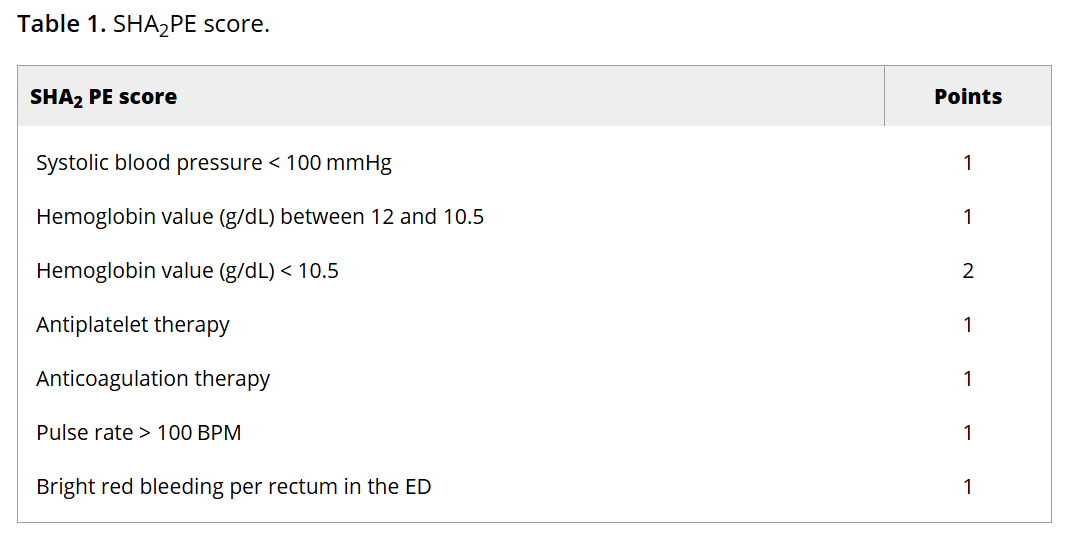
Lower GI bleed is a common reason for ED visits. This study aimed to validate a scoring system to identify low-risk LGIB pts who could be safely discharged from the ED.
The SHA2PE score incorporates characteristics and data that are commonly collected on patients with this complaint; readers can click through to see the scoring system. A score of less than or equal to 1 helps identify patients suitable for outpatient management, with a NPV of 98.3% (95% CI [97.2-99.1]) for predicting the need for hospitalization and acute intervention. However, the findings should be interpreted with caution given the relatively low prevalence of interventions within the study population.
Show Additional Information
Show References
Should we give a dose of antibiotics after intubating to reduce risk of VAP down the line? A multicenter RCT conducted in 2024 - the PROPHY-VAP Trial - found that a single dose of 2g ceftriaxone administered within 12 hours of intubation reduced VAP within the first week of hospitalization for patients intubated for airway protection due to TBI, stroke or SAH, with a VAP rate of 14% in the CTX group vs 32% in the VAP group (HR 0.60; 95% CI 0.38-0.95).
Click the link below for details and additional discussion
Show Additional Information
Show References
In 290 trauma patients diagnosed with dementia prior to injury, when compared to 3000 patients over age 65 without dementia and similar injury severity score, the dementia patients had a much higher rate of discharge to an institution instead of back to home living. This was particularly true of older women.
Show References
How much do you trust your plain film in the evaluation of elderly patients with traumatic hip pain?
Show Additional Information
Show References
BOTTOM LINE: It is critical to recognize and treat symptomatic hypocalcemia in pediatric patients.
Pediatric hypocalcemia has a variety of causes that should be considered. In the neonate congenital causes should be on the differential.
- In neonates, common causes include prematurity, infections, and maternal diabetes
- In infants and children vitamin D deficiency is most common, with rare causes including genetic etiologies, hyperparathyroidism and pseudohypoparathyroidism
Parathyroid hormone levels should be checked on all patients along with magnesium levels and ionized calcium.
An ECG should also be obtained for prolonged QTc.
Management is guided by acute symptoms (tetany, seizures, cramping, etc.) or other signs of critical illness (sepsis, trauma, etc.) in conjunction with low ionized calcium levels.
For symptomatic patients give 20 mg/kg of elemental calcium IV over a 10–20 min period
- 2 ml/kg of 10% calcium gluconate OR
- 0.7 ml/kg of 10% calcium chloride
For asymptomatic patient oral calcium supplements are typically given.
Failure to recognize concomitant hypomagnesemia may result in hypocalcemia that is resistant to treatment.
Disposition: Those children receiving IV calcium should be admitted with every 4-to-6-hour calcium levels and typically require ICU level admission. Children being monitored with oral supplementation can often be observed on a pediatric floor presuming there are no ECG abnormalities.
Show References
This article describes a paramedic run community health initiative to assist people with dementia transition to home after an ED visit. They describe:
“Persons living with dementia (PLWD) frequently use the emergency department (ED) for unscheduled care and experience significant challenges during the ED-to-home transition.
The Community Paramedic-led Transitions Intervention (CPTI) is a structured, coaching-based program delivered by community paramedics that includes a home visit and follow-up calls to support PLWD and care partners during the 30?days after ED discharge.”
Could your ED use a program like this to prevent readmissions?