Search
Pitfalls with PLR
- The passive leg raise (PLR) test has become a popular method to assess volume responsiveness in critically ill patients.
- PLR mobilizes a volume of approximately 150-300 mL and can be used in spontaneously breathing patients, those receiving positive pressure ventilation, or those with various arrhythmias.
- In order to properly perform the PLR, you must have a method to monitor cardiac output. (See previously pearl on 7/26/16).
- Pitfall: Simply monitoring arterial blood pressure alone is not a sufficient method to assess a positive PLR.
- Pitfalls:Risks of performing a PLR include increased intracranial pressure, reduced cerebral blood flow, and decreased pulmonary compliance.
Show References
Question
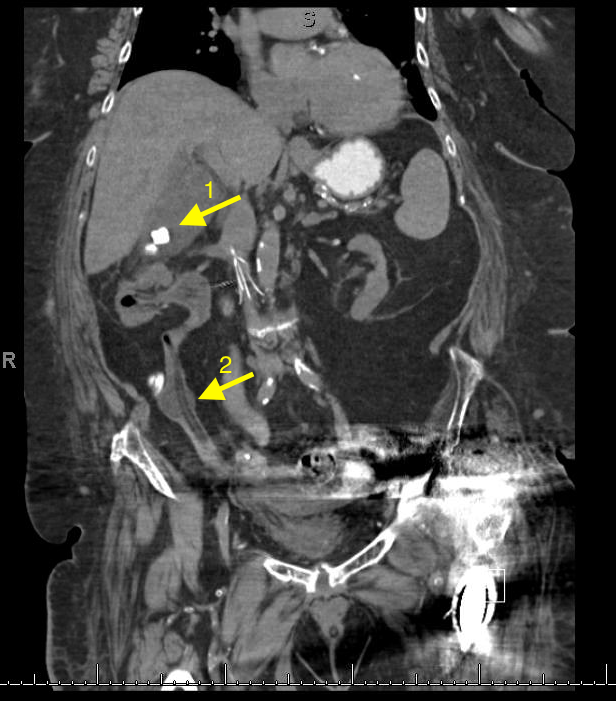
A 67 year old female with history of CVA, presented from a nursing home with RUQ abdominal pain and inablitiy to tolerate PO for 3 days. A CT scan of her abdomen was obtained. What is the diagnosis ?

Show Answer
Show References
Patellofemoral Syndrome Treatment options
Patients do best with a combined intervention (ie, exercise therapy, education, manual therapy and taping) plan or patellofemoral bracing may improve outcomes for people with patellofemoral syndrome and the subtype of patellofemoral osteoarthritis.
For for the ED, we can start NSAIDs, and then have them follow up with Physical Therapy, A sports trainer if in organized sports, or with a sports medicine physician/PCP. Physical therapy is targeted at strengthening the quadricep muscle particularly vastus medialis, which improves the patella’s tracking with knee flexion.
114 children with bronchiolitis had end tidal carbon dioxide (ETCO2) measured on presentation to the ED. The ETCO2 levels did not differ significantly between admitted and discharged patients. In the subset of admitted patients, there was no correlation with ETCO2 on admission and days of oxygen requirement or length of stay.
Bottom line: Initial ETCO2 does not predict outcome for patients with bronchiolitis.
Show References
Naloxone has been used to reverse opioid-induced respiratory depression for decades. The “standard” dose of opioid intoxication has been 0.4 mg. However, over the past decade, initial naloxone dose for opioid intoxication has evolved to recommend a lower initial dose (0.04 – 0.05 mg).
A recent article by Connors et al. reviewed 25 medical resources (internet, medical texts and study guides) of different medical specialties (internal medicine, medical toxicology, emergency medicine, pediatrics, anesthesiology, pain medicine and general medicine)
Findings:
- 12 medical resources (48%) recommend using 0.05 mg or less IV as an initial dose.
- 9 medical resources (36%) recommend using 0.4 – 0.5 mg or higher as an initial dose.
- Maximum dose also ranged widely from 2 to 20 mg.
Recent editions of emergency medicine text (Rosen’s and Tinitinalli) recommend using 0.04 – 0.05 mg IV in ED patients with history of opioid dependence. Higher doses of naloxone are recommended for non-opioid dependent/apneic patients.
However, history of opioid dependence is difficult to obtain in patients with opioid induced CNS/respiratory depression.
Administering 0.4 mg or higher dose may/can acute agitation or opioid withdrawal symptoms that can utilize more ED resources to calm agitated patient/management of withdrawal. Thus it may be prudent to use low-dose strategy (0.04 mg IV with titration) to minimize the risk of precipitating naloxone-induced opioid withdrawal/agitation.
Bottom line:
In opioid-induced respiratory depression/apneic patients:
- Ventilate with bag-valve mask for apnea/hypoxia
- Administer naloxone: 0.04 mg IV every 2 – 3 min until reversal of respiratory depression/hypoxia is achieved.
To make 0.04 mg naloxone solution:
- Dilute 1 mL of 0.4 mg naloxone with 9 mL normal saline in 10 mL syringe.
Show References
- Beware of the patient who can't open his/her eyes but is otherwise awake!
- This coma mimic is the result of eyelid apraxia, which is the inability to voluntarily open eyes despite intact frontalis muscle contraction and absent oculomotor dysfunction.
- This can be seen in injuries of the nondominant hemisphere (e.g. R MCA stroke), medial frontal lobe, bilateral thalami (e.g. bilateral thalami stroke), and brainstem (e.g. progressive supranuclear palsy).
- When asking these patients to open their eyes, they may use their forehead muscles to try and raise their eyelids.
During rapid sequence intubation (RSI) we endeavor to avoid positive pressure ventilation, prior to securing a definitive airway. As such, an adequate buffer of oxygen is necessary to ensure a safe apneic period. This process involves replacing the residual nitrogen in the lung with oxygen. It has been demonstrated that a standard nonrebreather (NRB) mask alone does not provide a high enough fractional concentration of oxygen (FiO2) to optimally denitrogenate the lungs (1). Even when a nasal cannula at 15L/min is utilized in addition to the NRB, the resulting FiO2 is not ideal. A bag-valve mask (BVM) with a one-way valve or PEEP valve has been demonstrated to provide oxygen concentrations close to that of an anesthesia circuit. But its effectiveness is drastically reduced if a proper mask seal is not maintained during the entire pre-oxygenation period (1). This is not always logistically possible in the chaos of an Emergency Department intubation.
A standard NRB with the addition of flush-rate oxygen appears to be a viable alternative. Recently published in Annals of Emergency Medicine, Driver et al demonstrated that a NRB with wall oxygen flow rates increased to maximum levels, rather than the standard 15L/min, provided end-tidal O2 (ET-O2) levels similar to an anesthesia circuit (2).
Show References
During rapid sequence intubation (RSI) we endeavor to avoid positive pressure ventilation, prior to securing a definitive airway. As such, an adequate buffer of oxygen is necessary to ensure a safe apneic period. This process involves replacing the residual nitrogen in the lung with oxygen. It has been demonstrated that a standard nonrebreather (NRB) mask alone does not provide a high enough fractional concentration of oxygen (FiO2) to optimally denitrogenate the lungs (1). Even when a nasal cannula at 15L/min is utilized in addition to the NRB, the resulting FiO2 is not ideal. A bag-valve mask (BVM) with a one-way-valve or PEEP valve has been demonstrated to provide oxygen concentrations close to that of an anesthesia circuit. But its effectiveness is drastically reduced if a proper mask seal is not maintained during the entire pre-oxygenation period (1). This is not always logistically possible in the chaos of an Emergency Department intubation.
A standard NRB with the addition of flush-rate oxygen appears to be a viable alternative. Recently published in Annals of Emergency Medicine, Driver et al demonstrated that a NRB with wall oxygen flow rates increased to maximum levels, rather than the standard 15L/min, provided end-tidal O2 (ET-O2) levels similar to an anesthesia circuit (2).
Show References
Question
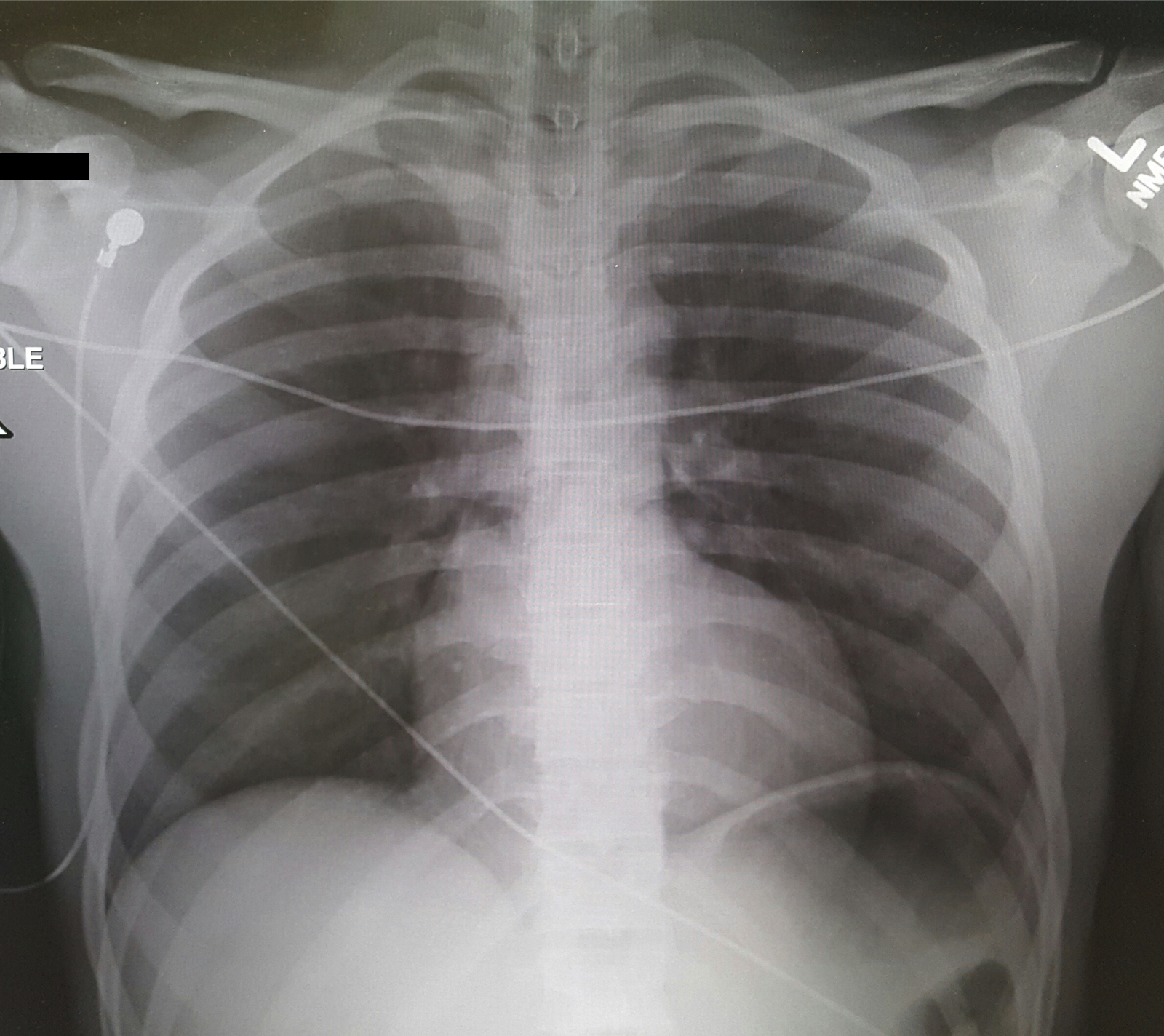
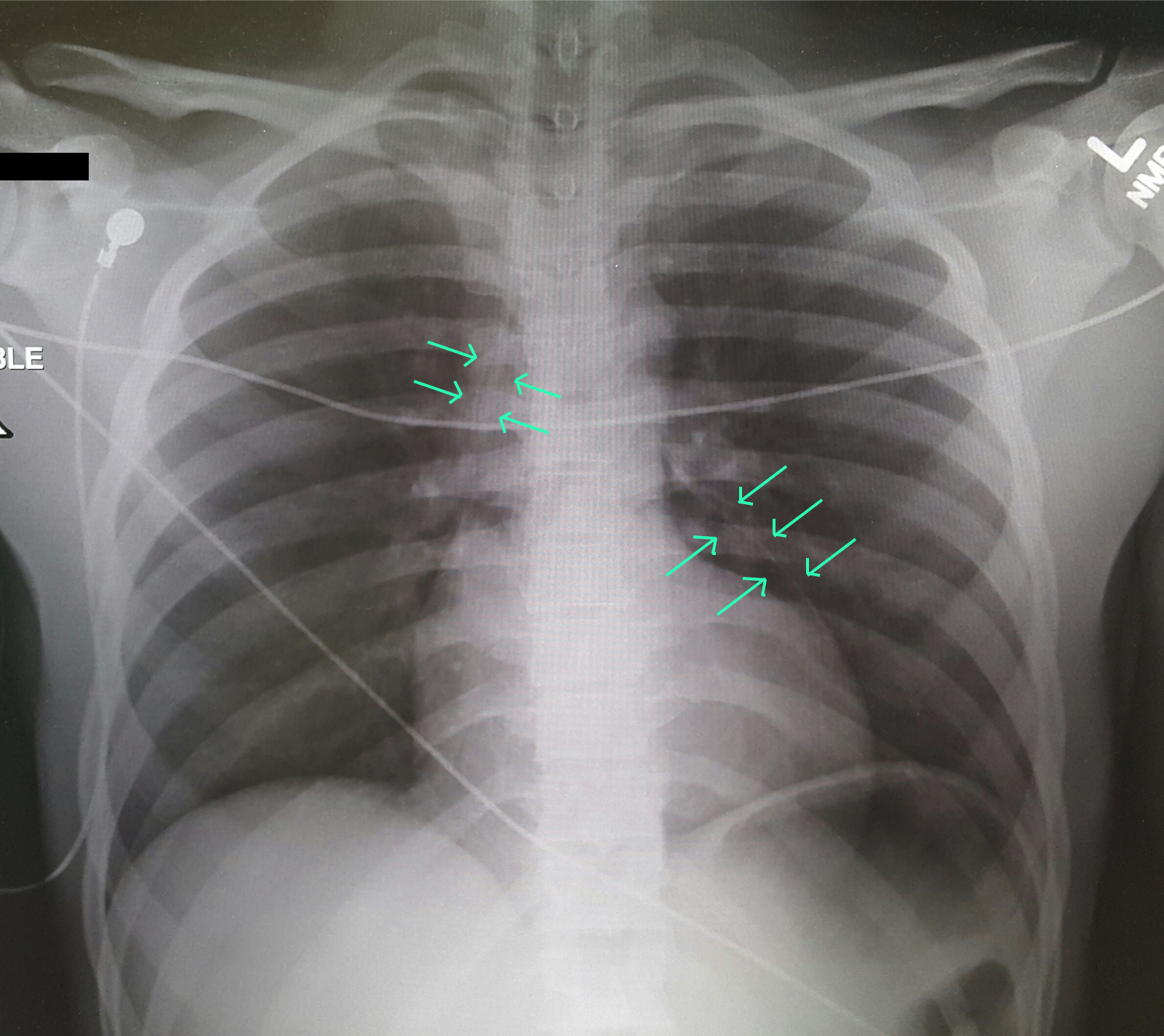
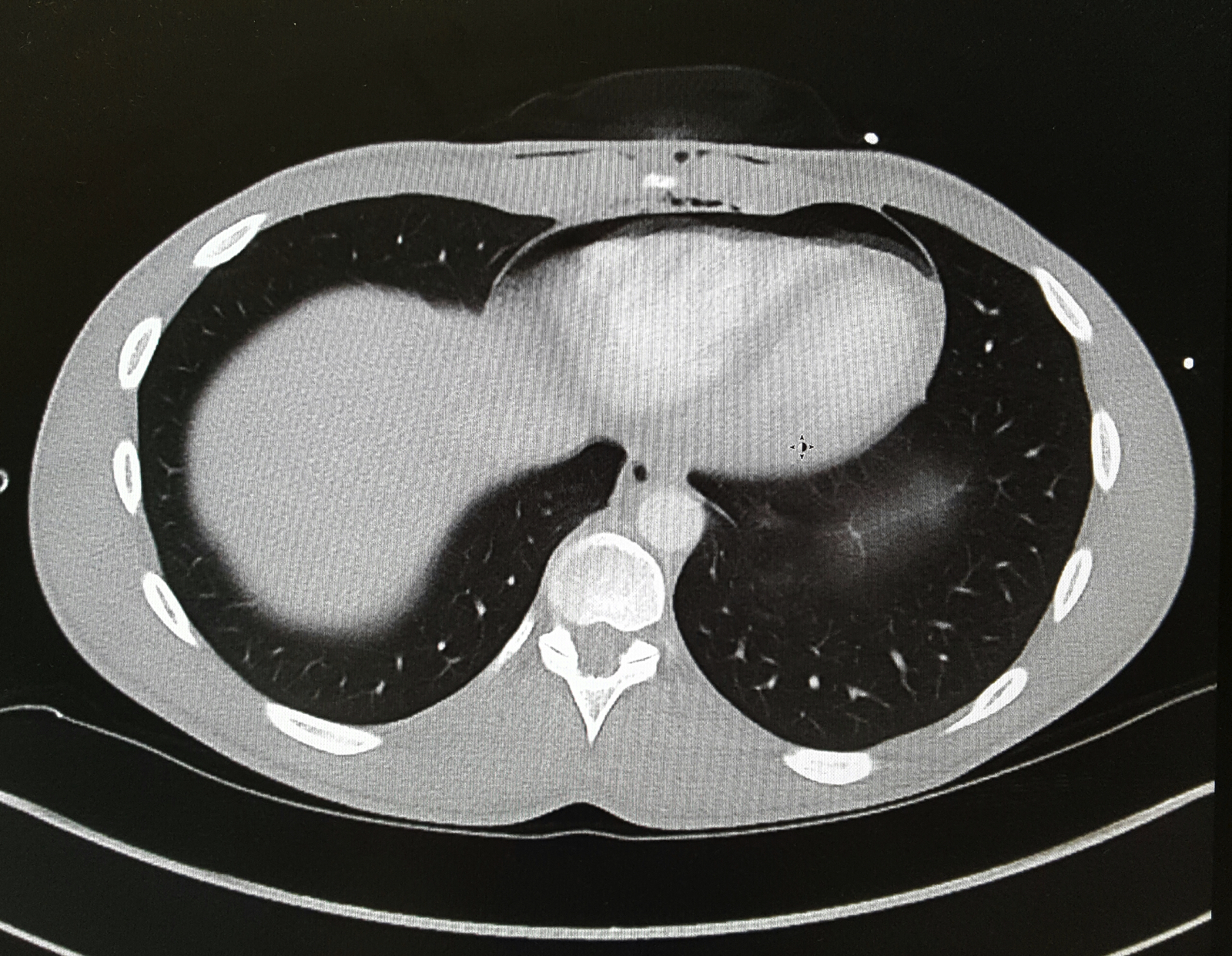
A 25-year-old male was brought in by EMS with a stab wound to the chest. What's the diagnosis?
Show Answer
Show References
Young athletes, especially around the age of puberty, are at higher risk for pelvic avulsion fractures
Often seen in sports that require sprinting, rapid changes in movement or jumping
Caused by sudden, forceful contraction of the muscles of the abdominal, the hip and thigh or the hamstring
Avulsion fractures can occur at many areas of the pelvis.
A mnemonic is: Alabama’s stoned rappers got ill hunting armadillos
· Iliac crest: Abdominal muscles
· Anterior superior iliac crest: Sartorius
· Anterior inferior iliac crest: Rectus femoris
· Greater trochanter: Gluteal muscles
· Lesser trochanter: Iliopsoas **(rare in adults)
· Ischial tuberosity: Hamstrings
· Pubic symphysis: Adductor group
http://roentgenrayreader.blogspot.com/2010/07/pelvic-avulsion-fractures.html
** Isolated nontraumatic avulsion fractures of the lesser trochanter in adults is a pathognomonic sign of metastatic disease
This site has some good images of common injury patterns
http://radiopaedia.org/articles/apophyseal-avulsion-fractures-of-the-pelvis-and-hip
Show References
Antipsychotic as a class has diverse range of toxicity. The atypical (2nd generation) antipsychotics are considered to possess less toxicologic manifestation compared to the typical (1st generation) antipsychotics - lower K channel blockade and minimum Na channel blockade properties. However, select atypical antipsychotics overdose can results in significant morbidity in addition to sedation.
Alpha-1 blockade (hypotension)
- Clozapine
- Olanzapine
- Quetiapine
- Risperidone
- Ziprasidone
Antimuscarinic effect (anticholinergic toxicity)
- Clozapine
- Olanzapine
- Quetiapine
Delayed rectifier K channel blockade (QT prolongation)
- Ertindole
- Ziprasidone
Bottom line: Although lethal overdose from atypical antipsychotics are rare, they can result in significant clinical toxicity when ingested alone or in combintation with other classes of medications.
Bottom Line:
- Cancers figure among the leading causes of morbidity and mortality worldwide, with approximately 14 million new cases and 8.2 million cancer related deaths in 2012.
- The number of new cases is expected to rise by about 70% over the next 2 decades.
- More than 30% of cancer deaths could be prevented by modifying or avoiding key risk factors
Show Additional Information
Show References
Question
--Aggressive BP management (SBP <140) in atraumatic intracerebral hemorrhage (ICH) does NOT signifcantly improve mortality or disability compared with traditional goal (SBP <180) [1]
--However, a lower goal (SBP <140) has been shown to decrease hematoma size and be safe compared to a higher goal (SBP <180) [2]
Show Answer
Show References
Prothrombin complex concentrate (PCC) and fresh frozen plasma (FFP) are used for INR reversal in patients on vitamin K antagonists (VKA) (e.g., warfarin) with life-threatening bleeding. Guidelines from the Neurocritical Care Society and Society of Critical Care Medicine recommend using PCC over FFP for patients with VKA-associated hemorrhage and an INR >=1.4.
New study-INCH trial:
- Multi-center, prospective, randomized, open-label trial comparing FFP IV 20 ml/kg + phytonadione IV 10 mg versus 4-factor PCC IV 30 IU/kg + phytonadione IV 10 mg
- Adult patients on VKA with intracerebral or subdural hemorrhage with INR >=2.0 were included. Patients with traumatic intracranial hemorrhage were excluded.
What they found:
- Analysis included 50 (23 FFP and 27 PCC) patients (trial was stopped early after a safety analysis)
- 2 (9%) patients in the FFP group and 18 (67%) patients in the PCC group achieved an INR <=1.2 within 3 hours (adjusted OR 30.6, 95% CI 4.7-197.9; p=0.0003)
- Hematoma expansion at 3 hours was higher in those treated with FFP than PCC (adjusted difference 16.9 ml, 95% CI 2.5-31.3; p=0.023)
- Time until INR <=1.2 was longer in the FFP group than the PCC group (1482 vs 40 minutes; p=0.050)
Application to clinical practice:
- Of note, FFP 30 ml/kg has been suggested to provide more complete coagulation factor correction (this trial used 20 ml/kg), and package inserts for PCCs recommend doses based on INR and weight (this trial used 30 IU/kg for all patients)
- Although the sample size was small, this study suggests that in patients with VKA-associated non-traumatic intracranial hemorrhage and an elevated INR, PCC may provide faster INR correction than FFP, and may additionally be associated with a smaller degree of hematoma expansion.
Show References
Zika virus and its transmission is currently an important infectious disease topic in the United States and the Western Hemisphere. With domestic spread in the Continental United States, and the likely further spread to other parts of the southern United States, continued vigilance by healthcare providers remains important.
What are the signs and symptoms of Zika?
Most common signs and symptoms are:
- Fever
- Rash
- Arthralgias
- Conjunctivitis (generally nonpurulent)
Other symptoms can include
- Myalgias
- Headaches
- Retro-orbital pain
- Gastrointestinal upset
Symptoms can generally last 2 to 7 days. Most individuals will have minimal or no significant symptoms and may not seek medical care. These symptoms are similar to other arboviruses, such as dengue or chikungunya. Potential serious complications include Guillian Barre syndrome.
Of course, the main concern remains infection of pregnant women and the impact that Zika has on the developing fetus, especially for the brain.
Show References
Ketamine for RSE?
- Up to 43% of patients with status epilepticus may progress to refractory status epilepticus (RSE).
- Propofol, midazolam, and barbituates are often recommended for patients with RSE.
- Importantly, all of these medications may be limited by hypotension and respiratory depression.
- Ketamine is emerging as adjuvant therapy for patients with RSE.
- The loading dose of ketamine ranges from 0.5 to 3 mg/kg, followed by a maintenance infusion of 0.3 to 4 mg/kg/h.
Show References
Show References
Ataxia is an important clinical sign of cerebellar pathology, but how is it actually described?
Stance ataxia: inability to stand with feet together for more than 30 seconds
Gait ataxia
Sensory ataxia: the first 2 elements, in addition to a positive Romberg sign
Truncal ataxia: oscillation of body while sitting or standing
Limb ataxia: functional impairment in performing actions such as writing or buttoning and improves with slowing down the movement
Dysdiadokinesia: impairment of rapidly alternating movement
Intention tremor: tested by finger-to-nose and heel-to-shin.
Dysmetria: pastpointing or undershooting on finger-chasing or shin-tap.
Dysarthria: irregular and slow speech with unnecessary hesitation
Nystagmus and other ocular disturbances, such as ocular flutter and opsoclonus.
The first 3 are present in both cerebellar pathology and loss of proprioceptive input, the rest are usually due to cerebellar pathology or ataxic syndrome.
Show References
Is it possible to have a patient present in diabetic ketoacidosis (DKA) with both negative serum and urinary ketone levels?
A case report published in American Journal of Emergency Medicine by Jehle et al provides a helpful reminder of this phenomenon (1). The degree of acidosis is directly related to the ratio of the various ketones/ketone metabolites: acetone, acetoacetate and beta-hydroxybutyrate present in the serum. The proportion of each respective substance is determined by the existing redox state in the blood. At any given time, acetoacetate and beta-hydroxybutyrate exist in an equilibrium dependent upon the ratio of NAD+ and NADH(fig.1). These substances freely convert with the assistance of the enzyme beta-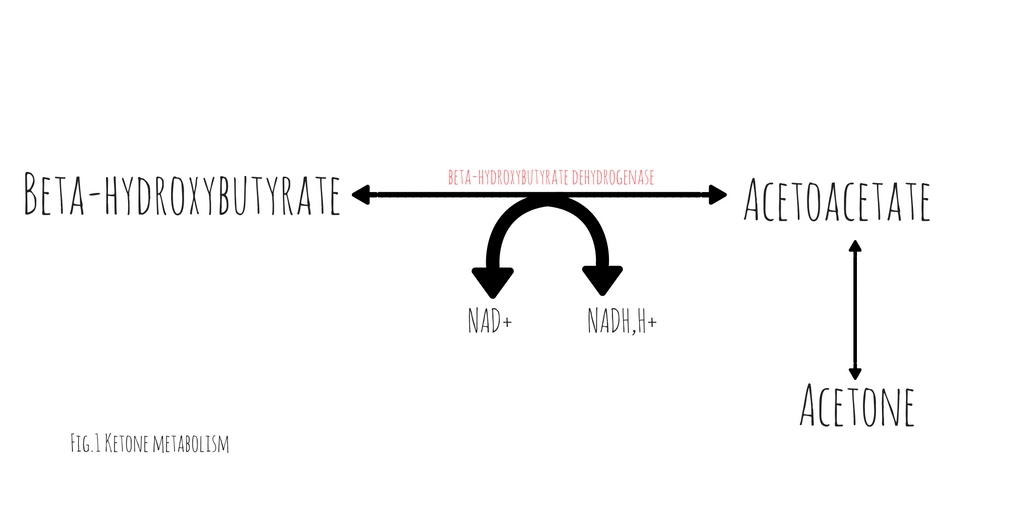 hydroxybutyrate dehydrogenase (2). This conversion requires the donation of a hydrogen atom from NADH. The balance between beta-hydroxybutyrate and acetoacetate, is determined by the ratio of NADH to NAD+. Acetoacetate will freely degrade into acetone through non-enzymatic decarboxylation. Early in DKA, acetoacetate is the most prevalent substance. As the disease progresses and the serum ratio of NADH to NAD+ increases, the proportion of beta-hydroxybutyrate rises, decreasing the quantity of acetoacetate and acetone.
hydroxybutyrate dehydrogenase (2). This conversion requires the donation of a hydrogen atom from NADH. The balance between beta-hydroxybutyrate and acetoacetate, is determined by the ratio of NADH to NAD+. Acetoacetate will freely degrade into acetone through non-enzymatic decarboxylation. Early in DKA, acetoacetate is the most prevalent substance. As the disease progresses and the serum ratio of NADH to NAD+ increases, the proportion of beta-hydroxybutyrate rises, decreasing the quantity of acetoacetate and acetone.
Traditional serum and urinary ketone assays react strongly to acetoacetate but neither reliably react with beta-hydroxybutyrate. Patients in whom the majority of their anion gap is filled by beta-hydroxybutyrate, urinary or serum ketone levels may be negative. In such cases, serum beta-hydroxybutyrate assays would be positive but are not universally available.
It is important to note, with resuscitation and insulin therapy, the ratio of NADH/NAD+ will start to normalize causing an increase in the quantity of acetoacetate. As the patient improves and the anion gap clears, the degree of ketones detected in the serum and urine will paradoxically increase.
Show References
According to the 4th International Patellofemoral Pain Research Retreat recently published in British Journal of Sports Medicine, the core criterion required to define Patelofemoral Pain (PFP) syndrome is pain around or behind the patella, which is aggravated by at least one activity that loads the patellofemoral joint during weight bearing on a flexed knee (eg, squatting, stair ambulation, jogging/running, hopping/jumping).
Additional criteria (not essential):
- Crepitus or grinding sensation emanating from the patellofemoral joint during knee flexion movement
- Tenderness on patellar facet palpation
- Small effusion
- Pain on sitting, rising on sitting, or straightening the knee following sitting
PFP is common in young adolescents, with a prevalence of 7–28%, and incidence of 9.2%.
Stay tuned for recommendations on treatment and diagnosis.