Search
A recent study in AJEM reviewed the utility of TXA in GI bleeding
This is a PRISMA?guided systematic review and meta?analysis of 7 RCTs (13,608 adults, 1976–2024) evaluating IV TXA vs placebo in acute gastrointestinal bleeding, including upper and mixed GI sources across multiple countries. The largest contributor is HALT?IT (Roberts et al.), which accounts for nearly 90% of participants.
-Mortality: No statistically significant reduction in all?cause mortality with TXA (OR 0.77; 95% CI 0.56–1.07, P = 0.12).?
-Rebleeding: TXA significantly reduced rebleeding events (OR 0.64; 95% CI 0.45–0.91, P = 0.01).?
-"Failure to control" bleeding: TXA reduced failure of hemostasis (OR 0.55; 95% CI 0.32–0.93, P = 0.03).
-Thromboembolic events: Random?effects model showed no significant difference (OR 1.28; 95% CI 0.51–4.51, P = 0.46), but fixed?effect analysis suggested a statistically significant increase (OR 1.28; 95% CI 1.07–1.55, P = 0.009), highlighting a possible thrombotic signal.?
-Transfusion and LOS: No significant reduction in blood transfusion requirements with TXA (OR 0.94; 95% CI 0.61–1.43, P = 0.76); length of stay and other resource metrics were variably reported and not clearly improved.
Take-Aways:
TXA may be reasonable as an adjunct in GI bleeding when the goal is to reduce rebleeding or “failure to control” bleeding, but current evidence does not support it as a mortality?reducing therapy.?
Given a potential increased risk of thromboembolic events, TXA should be used cautiously in patients with high baseline thrombotic risk, and always as part of a broader package including resuscitation and timely endoscopy rather than as a standalone intervention.
Show References
Last month, Mark Sutherland posted an overview of a new article investigating the use of personalized MAP targets in resuscitation for septic shock (1). Now, the authors of ANDROMEDA-SHOCK-2 (2) suggest a new multimodal approach to personalize resuscitation in septic shock that largely operates outside of the traditional focus on MAP and lactate.
In 2019, the ANDROMEDA-SHOCK Trial (3) suggested that capillary refill time (CRT) may be a better resuscitation in septic shock than lactate. Now, the same group is suggesting that a stepwise algorithm to guide resuscitation may provide more optimal and “personalized” results when compared to usual care for patients with abnormal CRT:
Tier 1: If CRT is abnormal, assess pulse pressure (PP) and DBP:
- PP (<40mmHg) OR DBP (>50mmHg)? Assess for fluid responsiveness and challenge with up to 1L IVF if fluid responsive.
- PP (>40mmHg) AND DBP (<50mmHg)? Increase norepinephrine (NE) for DBP >50mmHg, followed by assessment for fluid responsiveness and possible fluid challenge if CRT remains abnormal.
Tier 2: If CRT remains abnormal despite the above, use POCUS to assess for cardiac dysfunction.
- LV dysfunction? Trial dobutamine @ 5-75 mcg/kg/min (stop for HR > 120 or tachyarrhythmia, or if it doesnt help CRT)
- RV dysfunction? The authors recommend avoiding fluids, increasing pressors if needed, as well as decreasing PEEP, limiting plateau pressures, and/or proning the patient if they have ARDS
- If there is no cardiac dysfunction, assess for fluid responsiveness and fluid challenge if fluid responsive. Continue this cycle until CRT normalizes or there is evidence of harm (evidence of pulmonary edema, worsening oxygenation/ventilation, or high central venous pressure).
- If the patient is not fluid responsive, investigate for a history of HTN
- If they have a history of HTN, push MAP to 80-85 for 1h and see if it improves CRT (if not, revert back)
- If they do not, trial dobutamine @ 5 for 1h and see if it improves CRT (if not, DC dobutamine)
- If the patient is not fluid responsive, investigate for a history of HTN
- If CRT remains abnormal after all of this, move on to “rescue therapies” (high dose steroids, hemofiltration, ECMO).
The authors found that at 6 hours, following the protocol resulted in increased use of dobutamine, lower fluid balance, and similar CVP and MAP with lower lactate levels and CRT. They reported an improvement in their composite hierarchical outcome at 28 days, primarily driven by a shorter duration of organ support (vasoactives, mechanical ventilation, renal replacement therapy) and among sicker patients. No difference in mortality was observed between groups.
Food for Thought:
- CRT is a subjective assessment, and all participating clinicians in this study underwent mandatory training. Other, more objective measures that can be used to assess organ perfusion (lactate clearance, urine output, MAP) were excluded from this protocol.
- Fluid responsiveness was assessed using the “preferred technique by each center.” Suggested techniques included pulse pressure/stroke volume variation, change in VTI with passive leg raise, IVC variability, or change in CO with end expiratory pause.
- There was no standardization regarding the integration of vasopressin, and steroids were reserved as “rescue therapies” and considered at the same point as mechanical hemodynamic support.
- The effect of other inotropic agents (like low dose epinephrine) was not discussed.
Study Details:
- Setting: multicenter randomized control trial conducted in 86 ICUs across 19 countries
- Patients:
- >1450 adults from the ED, ICU, OR, or floor with septic shock based on Sepsis-3 criteria - suspected/confirmed infection + lactate >2 + pressor requirement to maintain MAP> 65 despite 1L+ IVF bolus.
- Patients with Child B or C cirrhosis, acute hematologic malignancy, severe ARDS, or anticipated surgery or HD within 8h of being diagnosed with septic shock, or who could not be enrolled within 4h of diagnosis were excluded. Pregnant patients were also excluded.
- Almost half had an abdominal source of infection, followed by respiratory and urinary.
- The median time to enrollment was 2h from meeting sepsis criteria
- Outcome: a hierarchical composite outcome using all-cause mortality, duration of vital support (vasoactives, invasive mechanical ventilation, or renal replacement therapy), and hospital LOS at 28d.
- The primary outcome was assessed in a hierarchical fashion using “wins” and “losses.” The intervention group “won” in 48.9% of cases, while the usual care group “won” in 42.1%, for a Stratified Win Ration of 1.16 (95% CI 1.02-1.33).
Show References
A large-scale retrospective study of 3.7 million children found an association between radiation exposure from medical imaging and a small but significantly increased risk of developing hematologic cancers (primarily leukemia).
-
Finding: Cancer risk increased with cumulative radiation dose
-
Dose-Response: For the highest exposure group (50 to <100 mGy), the Relative Risk (RR) for hematologic cancer was 3.59 compared to no exposure.
- Note: 13.7 mGy is roughly one head CT
- Note: 13.7 mGy is roughly one head CT
-
Attributable Risk: An estimated 10.1% of hematologic cancers in the cohort may have been attributable to medical imaging radiation, with CT scans being a major contributor.
-
Vulnerability: Children are more susceptible to radiation-induced cancer due to their heightened radiosensitivity and longer life expectancy for the cancer to manifest.
Take Away: Providers should critically assess the necessity of high-dose imaging like CT scans and use the lowest effective dose or possible alternative imaging (e.g. US, MRI, etc.) to prevent unnecessary cumulative exposure.
Show References
Summary
Objective:
The study aimed to determine how a brief educational intervention could enable emergency medicine (EM) residents to use point-of-care ultrasound (POCUS) effectively to diagnose and manage shoulder dislocations in the emergency department (ED).
Methods:
Conducted at an academic teaching hospital in Miami, Florida.
Twenty EM residents (PGY1–PGY4) with no prior shoulder ultrasound training participated.
Residents received <1 hour of in-service training, including a short lecture, video instruction, and hands-on practice using a Sonosite M-Turbo ultrasound device.
Over one year (2016–2017), residents prospectively enrolled 78 adult patients with suspected shoulder dislocation.
POCUS findings were compared with x-rays (the gold standard) for accuracy.
Time to diagnosis and reduction confirmation were recorded.
Results:
55 of 78 patients were diagnosed with dislocation; 53 anterior, 1 posterior, 1 inferior.
POCUS achieved 100% sensitivity and specificity for diagnosing and confirming successful reductions compared to x-ray.
Ultrasound results were available ~22 minutes faster for diagnosis and ~27 minutes faster for reduction confirmation than x-rays (p < 0.0001).
Residents across all training years performed equally well.
POCUS also identified 14 fractures (12 confirmed by x-ray, 2 seen only on ultrasound).
Discussion:
A short educational session enabled residents to accurately use POCUS for shoulder dislocation diagnosis and management.
POCUS reduced diagnostic time, avoided radiation exposure, and may improve ED workflow and patient comfort.
Findings support including shoulder ultrasound as a core component of EM training, filling a current gap in national ultrasound education guidelines.
Limitations:
Convenience sample and single-center design.
Some selection bias and inherent limitations of POCUS-based studies.
Conclusion:
Emergency medicine residents can learn to diagnose and manage shoulder dislocations with excellent accuracy after brief ultrasound training. POCUS should be integrated into EM residency curricula as a core skill for musculoskeletal emergencies.
- Nitrous oxide (N2O) aka “laughing gas”, used clinically for its psychotropic properties as an inhalational anesthetic, is one of the most abused inhalants for decades due to its unregulated wide availability and public perception that it is a safe high. Social media trends have popularized use by teens and young adults.
- Easily purchased online, in groceries stores, gas stations, smoke and vape shops it is used as a food processing propellant in steel aerosol containers like whipped cream and available in small canisters marketed as whipped cream chargers called “whippets”.
- Between January 1, 2014 - Dec 31, 2023, nitrous oxide nearly doubled in exposure rate with a total of 2,322 exposures reported to U.S Poison Centers. From 2010-2023, 1240 US deaths were reported between the ages of 15-74 attributable to nitrous oxide poisoning.
- Similar to Ketamine and phencyclidine, nitrous oxide causes antagonism at the NMDA receptor resulting in short lived reversible euphoria and sedation and analgesic effects through the K-opioid receptor.
- Nitrous oxide fatalities occur primarily due to asphyxiation and oxygen deprivation causing neurologic sequela, hypotension, arrythmias, and death. N2O depresses the sensation of shortness of breath so users may not seek fresh air.
- Chronic recreational N2O exposure impedes vitamin B12 function and causes a distinct neurological syndrome manifested by numbness, gait disturbances, loss of coordination, changes in mentation, and loss of bowel and bladder control, and hematologic abnormalities.
- On June 6, 2025, the FDA issued a public advisory warning consumers not to inhale nitrous oxide products due to potential for severe adverse events if used for recreational nonfood purposes.
Show Additional Information

Show References
We have all been there – an ED patient with circulatory shock requiring vasoactive medications and, therefore, an arterial line for accurate and close monitoring of the MAP and appropriate titration of the infusions. But does it save lives?
The recently published NEJM article by Muller et al. takes a look at noninvasive BP monitoring (NIBP) by cuff versus early arterial catheterization in patients with hypotension and evidence of tissue hypoperfusion:
- Open-label, pragmatic, parallel-group, noninferiority, multicenter RCT across 9 ICUs in France
- Adult patients enrolled within 24h of ICU admission, randomized to NIBP (n=506) or arterial line placement within 4h of enrollment (n=504)
- 15% of NIBP group received art line during study period as deemed necessary by predefined safety criteria (unable to get NIBP or SpO2, for ex)
- 50% septic shock, >90% medical patients, 90% on pressors at randomization
- Notable exclusions: BMI >40, high-dose vasopressors (total norepi tartrate* + epi infusion rate >2.5 mcg/kg/min)
- Findings:
- No difference in primary outcome of 28-day mortality (34.3% NIBP vs. 36.9% art line)
- No difference in 90 day mortality, 28-day ventilator, vasopressor, or RRT-free days
- More arterial puncture attempts in the NIBP group (742 vs. 269 per 1000 ICU days)
- No increase in arterial line-associated infections or ischemia
- More (8 vs 1%) hematoma or hemorrhage at art line site in arterial line group
- More patients in NIBP group reported serious pain/discomfort related to device (13 vs 9%)
Bottom Line: This trial indicates that in appropriately-selected patients with shock, such as those not on high doses of vasopressors, with BMI < 40 and an ability to consistently obtain NIBP measurements, early arterial line placement in the ED for vasopressor titration is unlikely to improve outcomes. It is important to note other potential indications for arterial line placement (severe hypoxia, inability to obtain reliable SpO2 with need for ABG monitoring, cardiac arrest, pain related to NIBP cuff monitoring, intracranial hemorrhage, etcetera) may still make arterial line placement in the ED prudent and better for overall patient care.
*France refers to norepi by the tartrate formulation dose, US refers to the base norepi dose (ratio is 2:1 tartrate: base).
Show References
POCUS can be performed at the bedside to evaluate for acute scrotal conditions, including testicular torsion and inflammatory processes such as epididymo-orchitis.
A high-frequency linear transducer is typically used to scan the scrotum in two different planes. Additionally, a coronal "buddy view"—displaying both testes side by side—can aid in comparing echogenicity and vascularity.
On B-mode imaging, both testicular torsion and inflammatory conditions may present with testicular swelling and decreased homogeneity. However, color and power Doppler imaging can help to differentiate:
-
Inflammatory conditions (e.g., epididymo-orchitis) typically show increased vascular flow on color and power Doppler.
-
Testicular torsion usually demonstrates reduced or absent flow in the affected testis. However, in cases of intermittent torsion-detorsion, vascular flow may appear preserved or even increased. In such scenarios, repeat Doppler imaging after one hour may help clarify the diagnosis.
Show References
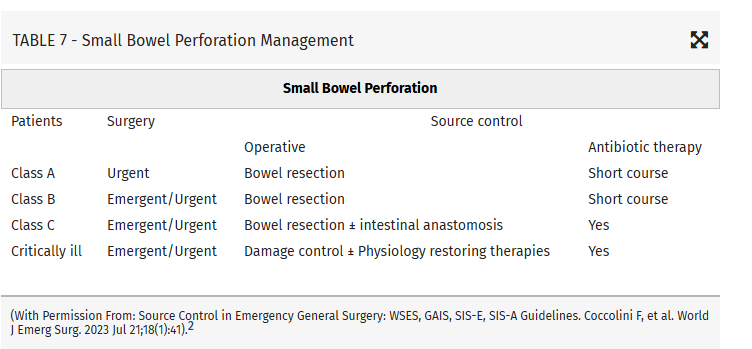
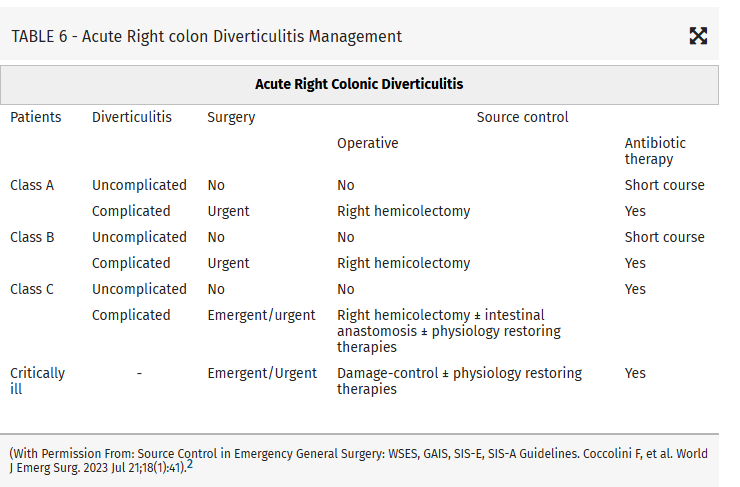
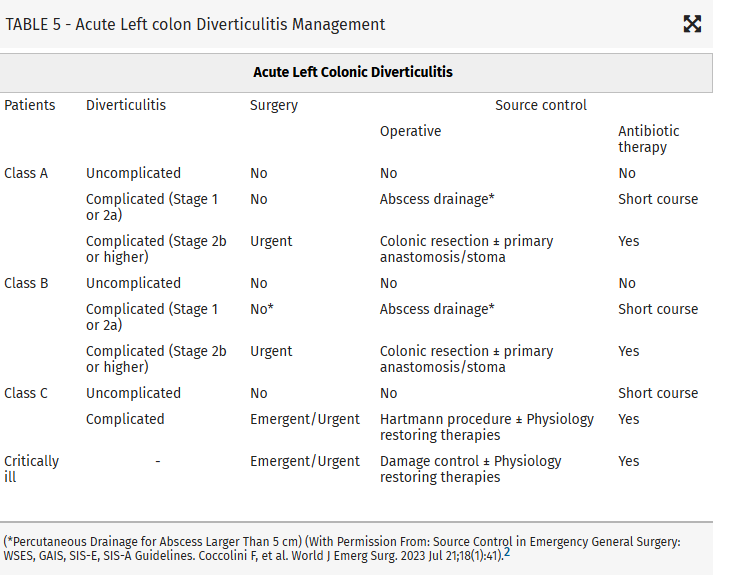
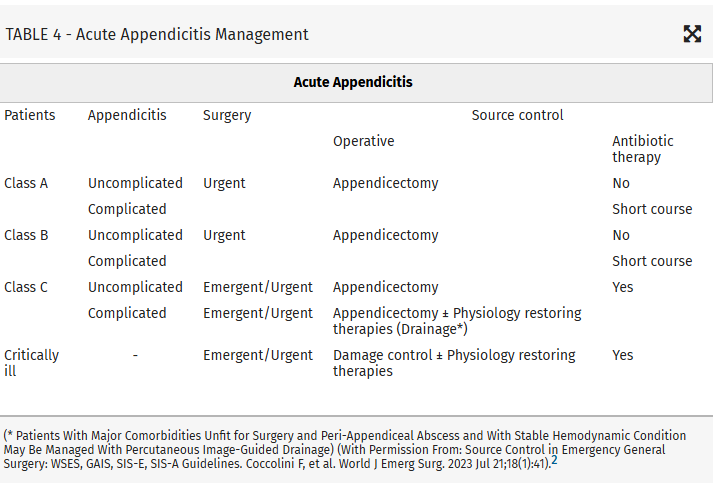
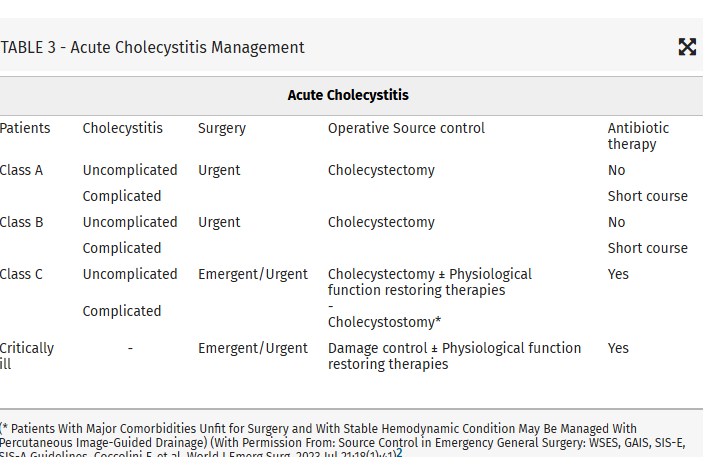
Intraabdominal infections leading to sepsis can come from cholecystitis, small bowel perforation, gastric perforation, left sided colonic diverticulitis, right sided diverticulitis and appendicitis. When to initiate source control and antibiotics is controversial. These authors propose breaking patient populations into three groups:
- Class A Healthy patients have no or else well-controlled comorbidities, and no immunocompromise, so that the IAI is the main problem.
- Class B Patients with moderate comorbidities and/or moderate immunocompromise are at risk of adverse outcomes due to their predisposing conditions, but are currently clinically stable. However, the IAI could rapidly worsen the prognosis.
- Class C Patients with severe comorbidities with advanced stages and/or severe immunocompromise, in which the infection worsens an already severe clinical condition.
From this they propose algorithms to treat these intraabdominal infections such as (note the different approach to right and left diverticulitis):
Show References
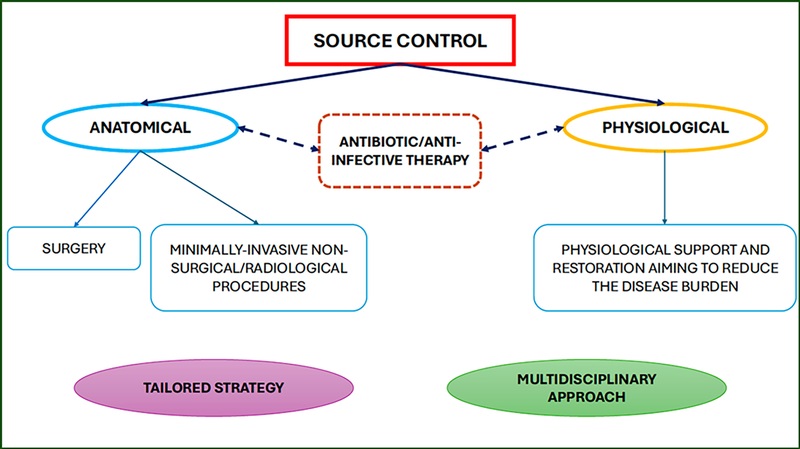
This article looks at source control as it relates to intrabdominal sources for sepsis. Key take aways are:
- They believe surgery is the best service to mange these complex patients in consultation with medicine, heme-onc, transplant, EM, etc. (Is that how it is done at your institution?)
- Source control should be both anatomic as well as physiologic (below)
- Timing of source control is controversial
- Antibiotic stewardship is still important even in these complex patients
Those at high risk of morbidity and mortality from intraabdominal infection associated sepsis include:
Mild–moderate immune deficiency: Elderly (according to the age and general status of the patient), Malnourished, Diabetic, Burns, Trauma, Uremic, Active malignancy, not on chemotherapy, HIV with CD4+ count >200/mm3, Splenectomized, Severe immune deficiencyAIDS HIV with CD4+ count <200/mm3, Transplant (solid organ, bone marrow), High-dose steroids (more than 20 mg/day prednisone), Malignancy on chemotherapy, Neutrophil count <1,000/mm3
High-risk population (medical or surgical causes)Low serum albumin concentration Older age Obesity Smoking Diabetes mellitus Ischemia secondary to vascular disease or irradiation Prolonged or delayed/late procedures
Show References
Comparing prescribing patterns from early 2000s to late 2010s in the National Hospital Ambulatory Medical Care Survey, these authors found we continue to under prescribe pain medications to non-white patients for traumatic injuries.
Show References
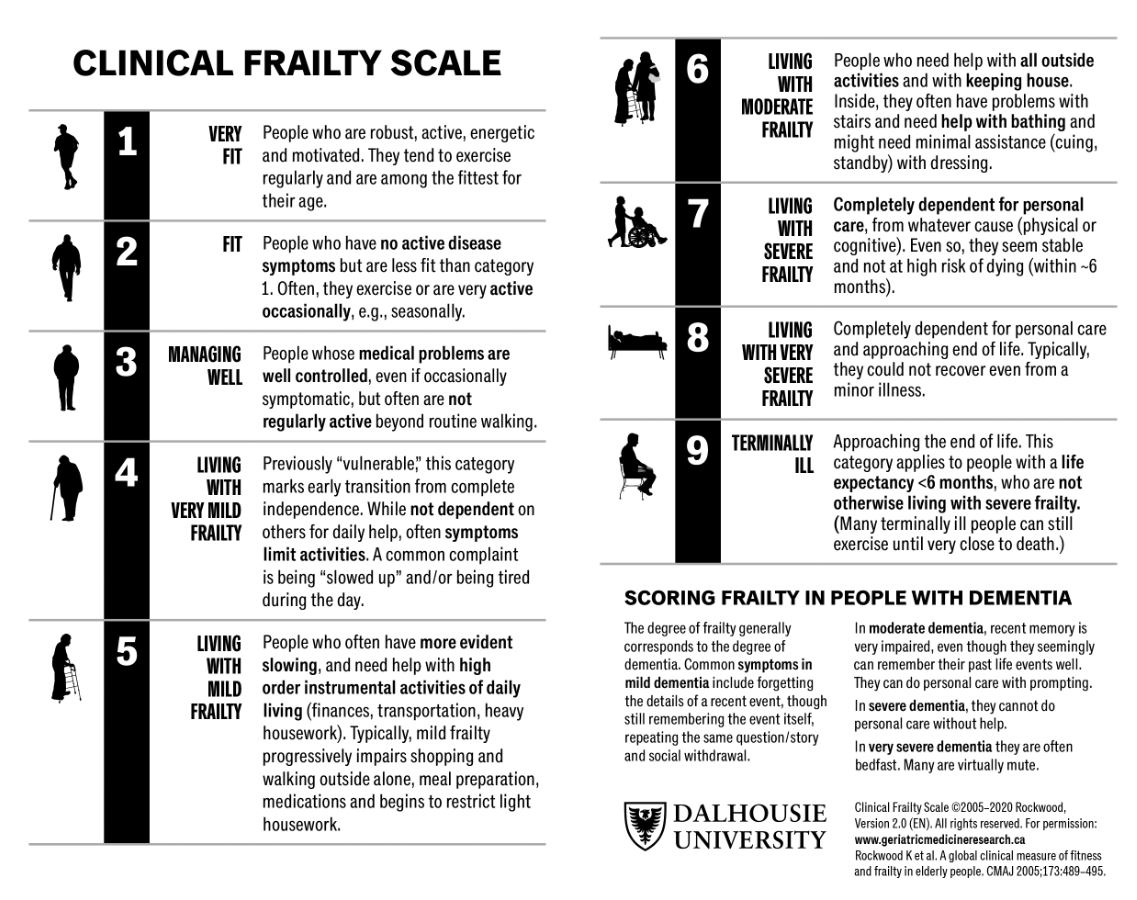
A prospective cohort of South Korean patients over 65 years admitted from the ED with critical illness had Clinical Frailty Scale (CFS) performed on them. Those with a high CFS had increased 3 month mortality. CFS helps us prognosticate morbidity and mortality in our older critically ill patients.
Show References
Food for thought on this Thanksgiving eve…
AI is rapidly being integrated into the practice of emergency medicine, as well as many other medical specialties. Similar to the adage, "you are what you eat," AI is what we feed it. See below for an introduction to the various levels of bias contributing to the machine learning process:
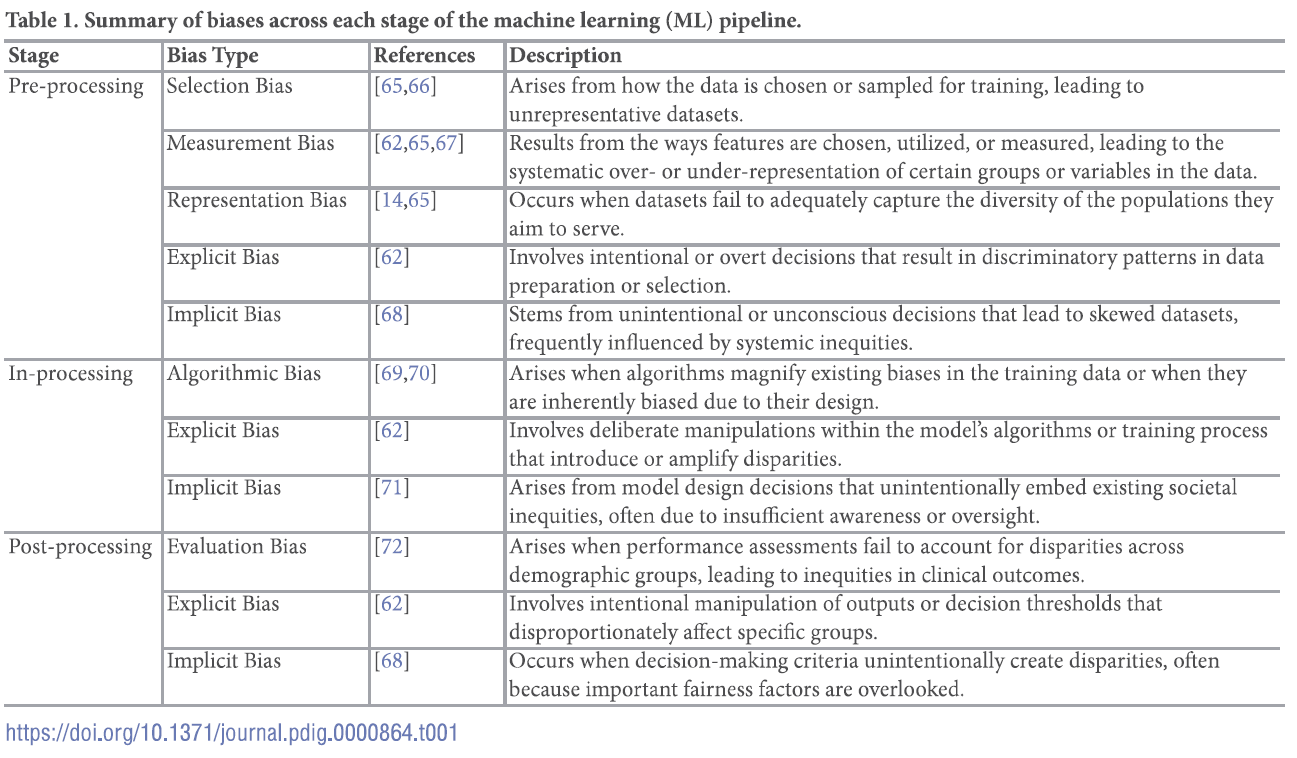
For a deep dive into the world of bias in AI, see referenced article.
Show References
Settings: this is a meta-analysis of 17 observational studies about boarding of critically ill patients in US Emergency Departments. All studies were from urban, academic centers.
Participants:
- There was a total of 407,178 patients, 194,814 (485) were boarding vs. 212,364 (52%) non-boarding patients.
- 355,86 (87%) patients were at centers with the presence of a resuscitation service.
- Ther was a mixture of critical illnesses: trauma (29.4 %), medical conditions (29.4 %) and mixed critical illness (41.2 %).
Outcome measurement: all cause mortality, as reported by the authors of the original studies.
Study Results:
- Overall, boarding patients were not associated with higher mortality, than non-boarding patients (Odd ratios 1.06, 95 % CI 0.94–1.19 p=0.383).
- Boarding patients were not associated with longer hospital length of stay (mean difference 0.38 days, 95%CI 0.94-1.50, P=0.51).
- However, among subgroup analyses, boarding patient population with mixed critical illnesses was associated with higher odds for mortality (OR 1.2, CI 1.04–1.4, p = 0.02 ) and longer HLOS (difference = 1.9, 95 % CI 0.81–3.1, I2 = 0 %, p = 0.001).
Discussion:
- All studies were observational so there was risk of bias and there was a presence of a small publication bias. This means that there were a few unpublished studies out there that showed that Boarding patients might have better outcomes.
- The findings that patient population with mixed illnesses were associated with higher odds for mortality, compared with Trauma-only or medical-only patients, might suggest that ED are not well equipped to take care of a wide spectrum of disease states. We seem to do better with populations with protocols such as sepsis, stroke, trauma.
- There was no clear consensus about how researchers approach this topic. A few studies did not even report their patient populations’ age (I cannot understand how these got published). Researchers used different thresholds for boarding, likely reflecting their institutional variabilities. There was quite a significant heterogeneity about patients’ acuity: some studies used SOFA, others used mSOFA.
- All of the studies were from urban academic centers so their results may not be applicable to non-academic centers which may not have many boarding issues
Conclusion:
Critically ill patients boarding in the U.S. Emergency Departments were associated with a non-statistically signi?cant increase in odds of mortality and hospital length of stay compared to non-boarded patients
Show References
The role of sodium bicarbonate in the treatment of severe acidemia has been controversial, with some studies suggesting no benefit, and others indicating that it may help reduce need for renal replacement therapy (RRT) and even improve mortality. The BICARICU-2 Trial was an open-label multicenter RCT conducted in France that evaluated the impact of a bicarb infusion among patients with metabolic acidosis and moderate to severe AKI.
There was no difference in 90 day mortality, but patients in the bicarb group were less likely to be started on RRT (38% vs 47% in the control group) using pre-defined criteria for RRT initiation, and had a 50% lower rate of bloodstream infections. Patients in the bicarb group who were started on RRT met criteria for RRT later than those in the control group (median 31h vs 15.5h).
Study Details:
Patient Population:
- SOFA score >4 OR arterial lactate > 2mmol/L within 48h of ICU admission
- Metabolic acidosis, defined by pH < 7.2, HCO3- < 20mEq/L, and PaCO2 < 45mmHg
- Moderate to severe AKI, defined as Cr >2.0 x baseline or UOP < 0.5 mL/kg/h for >12h.
- Patients with severe baseline CKD, ketoacidosis, intoxication with exogenous acids (metformin, salicylate, methanol, ethylene glycol), or ongoing bicarb losses via GI or urinary tracts were excluded.
- The presumed etiology of acidemia was septic shock in over half of included patients, and over 75% were on vasopressors.
Intervention:
- 4.2% bicarb infusion administered in 125-250 aliquots with a target pH >7.3, though not to exceed 1L/500mEq within 24h.
- The intervention continued for a maximum of 28d or until ICU DC.
- Patients in the intervention group received a median of 750mL in the first 48h.
RRT Triggers:
- Immediate: K > 6.5mEq/L with EKG changes or cardiogenic pulmonary edema with no UOP and hypoxia
- 24h after enrollment: UOP <0.3 Ml/kg/h over 24h, pH <7.2 despite resuscitation, K > 6.5 MEq/L.
Show References
Treatment of Staphylococcus aureus bacteremia has traditionally required several weeks of intravenous antibiotics. This approach carries medical risks, such as catheter-associated infection or thrombosis, as well as significant social and financial burdens for patients. Dalbavancin, a long-acting intravenous lipoglycopeptide with activity against S. aureus (including MRSA), has been proposed as a more convenient alternative. This study evaluated the efficacy and safety of dalbavancin compared with standard therapy for S. aureus bacteremia.
Two hundred adults were enrolled in this open-label, randomized clinical trial, which was conducted in the United States and Canada. After blood cultures cleared, participants were randomized to complete therapy with dalbavancin (administered on Days 1 and 8) or with standard treatment (cefazolin for MSSA and vancomycin or daptomycin for MRSA).
The primary outcome was the Desirability of Outcome Ranking (DOOR) at Day 70, incorporating five domains: clinical success, infectious complications, safety events, mortality, and health-related quality of life.
Dalbavancin was not superior to standard therapy for treating S. aureus bacteremia, and adverse events were similar between groups. A key strength of this study was the inclusion of people who inject drugs, a population at high risk for S. aureus bacteremia and often underrepresented in trials. A major limitation was that the DOOR metric did not account for important social and economic factors, such as disposition (home versus skilled nursing facility), caregiver burden, or treatment cost.
Key Takeaway: Dalbavancin may be a suitable alternative to traditional therapy for Staphylococcus aureus bacteremia, offering less frequent dosing and a shorter treatment course. Further research is needed to identify which patients benefit most and to evaluate its impact on social and economic factors such as discharge disposition, caregiver burden, and treatment costs.
Show References
In 252 mild traumatic brain injury patients seen at 3 level I centers that were given the Rivermead Post Concussion Symptoms Questionnaire within 24 hours of arrival, 3 month post concussive symptoms were significantly correlated with their score on the questionnaire. This questionnaire take 3 minutes to complete. This may be helpful in prognosticating who will have post-concussive symptoms and who will need additional follow up.
Show References
Turf Toe:
Increased recent attention due to injuries in high profile athletes
Sprain of the first MTP joint
Mechanism: Forced hyperextension of the great toe (most common)
https://briandorfman.com/wp-content/uploads/2015/11/b_12_3_6a.jpg
{kind=link}
Causes injury to the MTP joint capsule and surrounding ligaments
Presents as pain, swelling, discoloration, tenderness to palpation, possible joint laxity
Pain with active and passive ROM (both flexion and extension)
Graded 1-3 (Sprain, partial rupture, significant/complete rupture)
Most commonly seen in athletes who compete on artificial turf.
More rigid than natural grass
Synthetic surfaces do not release cleats as easily as natural grass
Improved synthetic surfaces perform more similar to natural grass
Much higher incidence in games vs practices.
In football, quarterbacks and running backs at highest risk
Between 30 and 45% of professional football players claim that they have experienced a turf toe injury, with over 80% of those injuries occurring on artificial turf
The combination of more rigid synthetic surfaces and lighter, more flexible shoes, increase risk of hyperextension injuries
Treatment: usually non operative
Rest/ice/taping after acute swelling decreased/stiff sole shoe/crutches/NSAIDs.
Consider walking boot or short leg splint for severe injuries
Less than 2% of injuries require surgery
Children account for up to 20% of emergency department visits. In the US, up to 90% of children’s visits to emergency departments are to general EDs. The weighted pediatric readiness score (WPRS) was developed to assess the level of readiness of emergency departments to care for pediatric patients. The last assessment was in 2013 showed a mean score of 68.9. High readiness scores have been associated with decreased mortality. The same holds true for children with injuries presenting to trauma centers. The higher the WPRS score, the lower the risk of in hospital death. There was no difference if the patient presented in cardiac arrest. A 10 point increase in WPRS is associated with a lower odds of potentially avoidable transfers in both trauma and medical patients. More recent data has been collected, but has not yet been published. More information on pediatric readiness (for hospitals and EMS) can be found at: https://emscimprovement.center/domains/pediatric-readiness/.
Bottom line: Being Pediatric Ready improves the care of children.
Show References
In reviewing the limited literature available, the authors found that fascia iliaca blocks did not improve mortality but did improve hospital length of stay, decreased opiate use, and decreased delirium rates. More research is needed, however this tool should be added to our multimodal pain control toolbox.
Show References
Early defibrillation is a key step in the cardiac arrest chain of survival. Public Access AEDs may be available more readily than waiting for first responders. Outside of simple awareness of where AEDs are located, there are newer ways to become aware of public AEDs near a cardiac arrest including cell phone apps or information given by 911. A British study showed that only 5.9% of AEDs were within 100 meters of the patient and 35% were within 500 meters. The distance between the AED and arrest may be a barrier for bystander AED use. This study looked to determine the time required to retrieve an AED and they hypothesized that a distance > 400 meters would be longer than the EMS response times.
This study used 15 women and 15 men to perform different runs in various environments in different seasons, retrieving AEDs at 200m through 600m and bringing it back to the patient. In these scenarios, only the 200m distance (400 m round trip) times were deemed to allow enough time to apply and use the AED prior to EMS arrival. Barriers to AED retrieval included traffic lights, cars, weather and pedestrians.