Search
21-40 of 310 results by Robert Flint
A narrative review of literature involving older patients and constipation found:
“Major contributing factors include physical inactivity, sarcopenia, dehydration, inappropriate defecation posture, and polypharmacy, particularly opioids and anticholinergic agents. Importantly, these factors interact through the brain–gut–microbiota axis, contributing not only to gastrointestinal dysfunction but also to systemic outcomes such as frailty, cognitive decline, and increased healthcare burden, thereby supporting a multidimensional disease framework.”
It isn’t as simple as adding a laxative.
Show References
The article outlines how instead of looking at medications as the cause of symptoms, we often add more medications to treat the medication induced symptoms. Here is an example of how we get to polypharmacy in older patients
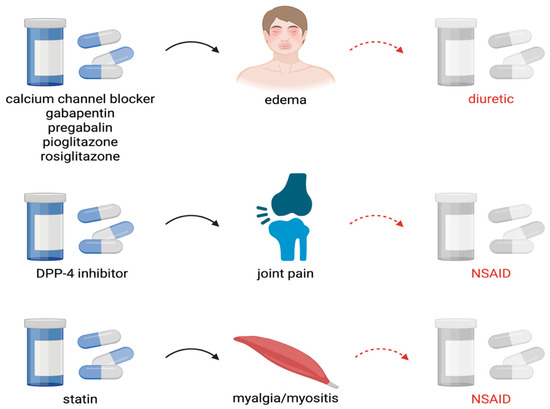
Show References
Body armor/ bullet resistant vests used by law enforcement are designed to stop penetration by handgun rounds. These rounds have less velocity than rifle rounds. When caring for someone who has been shot while wearing body armor, verify no penetration has occurred and then look for blunt injuries such as rib fractures, liver injuries, pneumothorax, cardiac contusion, vertebral injury, etc. Behind Armor Blunt Trauma (BABT) is the technical term for injuries caused by the transfer of kinetic energy that occurs when these vests are struck.
Show References
This narrative review of the trauma literature looking at chronic pain after trauma found:
- Chronic pain occurs in 30–70% of trauma survivors, with prevalence varying by injury type.
- Key risk factors include female sex, younger age, pre-existing pain, psychological distress, and social disadvantage.
- Validated prediction models are available for musculoskeletal trauma
- Thoracic trauma is under represented in the pain literature, is often underrecognized, and less protocols are available for treatment
- Thoracic pain typically occurs through intercostal nerve damage and persistent pain following thoracic injury
- The authors suggest “A trauma-specific, biopsychosocial approach is key to reducing chronic pain and improving recovery.”
Show References
This German retrospective review of 1500 level one trauma center patients (ICU level or ISS over 9) found obesity was an independent predictor of ARDS, multisystem organ failure, and sepsis but not pneumonia or mortality.
Show References
This German retrospective study compared the prehospital use of ultrasound by trained paramedics and compared their findings to in-hospital diagnosis and image results. The authors found:
“Diagnostic accuracy, defined as the concordance between prehospital POCUS-based working diagnoses and final in-hospital diagnoses, was particularly strong for lung ultrasound (pneumothorax, pulmonary edema, pneumonia and pleural effusion; sensitivity 91.7%, specificity 100%) and eFAST (sensitivity 100%, specificity 96.5%), while for the abdominal ultrasound examinations, the specificity was 70% and sensitivity was 71.43%.”
This study sets the stage for future prospective work looking at prehospital US use by paramedics.
Show References
This systematic literature review looking at gender differences in trauma care reveals:
- Women were older with more low-energy trauma than men.
- Women were more likely to suffer from pelvic and spinal cord injuries.
- Women were more likely to be under-triaged and under-treated.
- Sex/gender-based differences in mortality were inconsistent across studies.
- Adjusted mortality appeared similar between women and men
Show References
A modified 2 round Delphi study was used to create 57 learning objectives in geriatric care for European prehospital providers. Based on in-hospital learning objectives and literature, these experts came up with what appears to be a very reasonable and helpful list of education objectives for pre-hospital providers that could easily apply to emergency medicine learners as a whole. Here is their table:
https://link.springer.com/article/10.1186/s13049-026-01550-3/tables/3
Show References
In this retrospective cohort study looking at splenic injury management and outcomes in the UK, patients over age 65 had much higher mortality and were more often managed conservatively (vs splenectomy or embolization) despite having a lower splenic injury grade and lower overall injury severity score compared to those under 65. Many factors are possible here including frailty, reluctance to intervene in older patients, and lower mechanism of injury bias away from evaluation and management.
Show References
Looking at trauma patients evaluated at a major trauma center before and after EMS switched from semi-rigid to soft cervical collars for immobilization found no difference in adverse outcomes. Add this to the mounting evidence that our current practice of spinal immobilization may not offer any benefit.
Show References
Bradycardia accompanying hypotension can be found in spinal cord injury (loss of autonomic reflex), beta blocker and calcium channel blocker overdose, intrinsic cardiac electrophysiologic derangement, and, often forgotten, intrabdominal hemorrhage. In the appropriate setting (blunt trauma, ruptured ectopic pregnancy), bradycardic hypotensive patients should be considered the same as tachycardic hypotensive patients and get a work up and treatment focused on Hemoperitoneum.
Show References
Using a database of 300,000 patients and applying a predictive measure for mortality, these authors found that patients over 66 with a high likelihood of 6 month mortality at the time of presentation were more likely to be admitted to an ICU when they presented to an ED. The authors conclude there is much work to be done regarding discussion of goals of care based on this information.
Show References
Looking at a national database, this study concluded the use of low titer O whole blood during trauma resuscitations was increasing at level one centers but not at level 2 and 3 centers. Is this a representation of the national blood supply as whole blood is harder to stock? We need to understand this trend to assure equal and appropriate care to trauma patients across the country.
Show References
Another study, this one from New Zealand, showing older trauma patients with similar injury severity score had less trauma team activations and higher mortality.
Show References
This case report reminds us that vasculitis is an inflammatory process that attacks blood vessels leading to organ dysfunction. The etiology can be a hypersensitivity reaction (think drugs) or an IgA mediated process secondary to infection (Strep or Mycoplasma). In this case, concomitate use of NSAIDS (very common etiology of hypersensitivity) and Mycoplasma lead to vasculitis. Treatment ranges from supportive care, to steroids to immunosuppressive agents such as azathioprine.
Show References
Of 925 ED headache patients in this meta analysis comparing extrapyramidal side effects of bolus vs. continuous infusion of metoclopremide the majority of the reactions occurred in the bolus group.
Show References
When compared to saline(!) trauma patients with a high injury severity score who received ketamine via pca for pain control had better quality of life indicators at 1,3, and 6 months post injury.
Show References
Bottom Line: arrival temperature had no prognostic value in non-septic older patients. Hypothermia in sepsis, but not fever, predicted mortality.
Show References
In a single level 1 trauma center there were 274 patients age over 55 evaluated for falls in a one year retrospective period. Their blood toxicology was reviewed for presence of alcohol, opioids, benzodiazepines and cannabinoids. The authors found:
“detection rates were 21.2% for opioids, 18.6% for ethanol, 13.9% for benzodiazepines, and 9.1% for cannabinoids. Injuries identified included 16.4% spinal fractures, 9.5% extremity fractures, 7.7% hip/thigh/pelvic fractures…In this study, nearly 20% of adults 55+ presenting for fall-related trauma recently used substances that impair psychomotor function.”
An area for injury prevention research and intervention would be to screen patients over age 55 for substance use, consider prescribing patterns in this age group (benzodiazepines) , and discuss with patients fall risk avoidance.
Show References
A case report on use of the abdominal aortic and junctional tourniquet in a 27 year old female with hemorrhagic shock secondary to a pelvic fracture after a 10 meter fall demonstrated improved blood pressure and stabilized vasopressor use prior to operative intervention. This device has been used in battlefield situations, however very few reports of civilian use exist. Much more data is needed, however, it is a device to be aware of for future use.
