Search
From 2010-2014 ED visits in the US for injuries from trampoline parks (TPI) increased from 581 visits per year to 6932 visits per year. There was no change in the number of injuries related to home trampoline use. TPI were more likely to involve the lower extremity, be a dislocation and warrant admission and less likely to involve the head.
Bottom line: TPIs are increasing and have a different injury pattern compared to home trampolines.
Show References
In pediatric population, small dose or single pill ingestion can potential result in severe or lethal toxicity.
Clinicians should be mindful of potential toxicity following xenobiotic exposure (below) in pediatric population, especially under the age of 5 years old, even if the patient may initially appear asymptomatic.
- Benzocaine
- B-adrenergic antagonist (sustained release)
- Calcium Channel blockers (sustained release)
- Camphor
- Clonidine
- TCAs
- Diphenoxylate/atropine (Lomotil)
- Toxic alcohol (methanol or ethylene glycol)
- Methylsalicylate
- MAO-Is
- Opioids
- Phenothiazines
- Quinine or chloroquine
- Sulfonylureas
- Theophylline
Suspected ingestion of above medications/xenobiotics may warrent observation up to 24 hours in asymptomatic pediatric population.
July 2016 was the hottest month ever recorded. As the temperature of the planet continues to rise, changes in infectious disease patterns of transmission are likely to occur. Many formerly exotic diseases, such as Zika, West Nile, malaria and cholera are spreading to new areas. Some of these are now found in the United States. Below is a table (from M. L. Wilson) that exemplifies how environmental changes can impact infectious diseases.
Bottom Line: Remain vigilant for unusual infectious diseases, especially among travelers. However recognize that many diseases have the potential to spread to the U.S., especially considering ongoing environmental changes.

Show References
47yo M chef presents to your ED with 2 days of worsening left hand pain after sustaining a puncture wound to hand at work. The hand is red and swollen and he complains of pain. Interestingly, his index and middle digits are in an ABducted position at rest.
Collar Button Abscess
Web space infection of the palmer AND dorsal hand
The Palmer aponeurosis prevents volar extension (but promotes dorsal encroachment)
The pus spreads between the MC bones and erupts dorsally....creating a DORSAL abscess.
Loss of palmer concavity is seen.
ABduction of the adjacent digits, resulting in a "V" configuration with the apex pointing to the site of infection. This would not happen from simple pus in the dorsal space!
Can be missed if only focused on the dorsal hand. The palm will show the original injury (splinter, cut, foreign body)
Treatment is urgent surgical drainage.
http://www.eplasty.com/article_images/eplasty16ic06_fig1.gif
Show References
Question

Show Answer
Show References
Attachments
Zika Virus-associated GBS
- Zika virus has been shown to trigger Guillain-Barre Syndrome (GBS) at a rate similar to Campylobacter jejuni infections.
- In patients with Zika virus-associated GBS, neurologic deterioration has been rapid, with approximately 33% of patients developing respiratory distress.
- For patients who have required intubation, the duration of mechanical ventilation and length of ICU stay has been very long.
- Consider Zika virus-associated GBS in patients with muscle weakness, facial palsy, or paresthesias in the setting of a travel or exposure history to the virus.
Show References
Amiodarone 150 mg IV over 10 minutes and procainamide IV 20-50 mg/min (up to 17 mg/kg) are two antiarrhythmic medications recommended in the American Heart Association (AHA) Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care for stable wide QRS complex tachycardia. [1]
What they did:
Multi-center, prospective, randomized, open-label trial comparing the incidence of major cardiac events in the acute treatment of hemodynamically stable patients with wide QRS monomorphic tachycardia (presumed to be VT) using amiodarone 5 mg/kg IV infused over 20 minutes versus procainamide 10 mg/kg IV infused over 20 minutes. [2] The study period was 40 minutes, starting from the beginning of the infusion.
What they found:
- Analysis included 62 (n=33 procainamide, n=29 amiodarone) patients from 16 hospitals
- Fewer patients treated with procainamide experienced major cardiac events during the study period compared to those who received amiodarone (9% vs 41%; OR =0.1, 95% CI 0.03-0.6; P=0.006). The most frequent adverse cardiac event was severe hypotension requiring electrical cardioversion.
- Termination of VT occurred more frequently in patients treated with procainamide (67% vs 38%; OR =3.3, 95% CI 1.2-9.3; P=0.026).
Application to clinical practice:
- Medication doses and patient weights are not reported in the results. A comparison of the doses used in the PROCAMIO study to those recommended in the AHA guidelines for a 70 kg and 100 kg patient are as follows:
- Procainamide:
- 70 kg patient would receive procainamide 35 mg/min for 20 minutes. This is in the middle of the dose range recommended by the AHA.
- 100 kg patient would receive procainamide 50 mg/min for 20 minutes. This is the upper limit of the dose range recommended by the AHA.
- Amiodarone:
- 70 kg patient would receive amiodarone 350 mg over 20 minutes. This is approximately equal to administering 2 doses of 150 mg at the infusion rate recommended in the AHA guidelines.
- 100 kg patient would receive amiodarone 500 mg over 20 minutes. This is approximately equal to administering 3 doses of 150 mg at an infusion rate over 1.5 times higher than that recommended in the AHA guidelines.
- Procainamide:
- The study size was small, and depending on patient weights, it is possible that amiodarone dosing was more aggressive compared to doses commonly used in the US. However, the results suggest that procainamide could offer improved safety and efficacy over amiodarone for stable wide QRS tachycardia.
Show References
Drug-induced hypoglycemia is an often severe and symptomatic. It is a potentially preventable cause of significant morbidity. In one large study, it accounted for 23% for hospital admissions due to adverse drug events and 4.4% of overall admissions. The majority of hypoglycemic events occur with insulin and sulfonylureas. However, multiple drugs can affect glucose homeostasis and have been cited to cause hypoglycemia in therapeutic dose alone or in combination with other medications or illness. Factors that predispose to low blood sugar include reduced food intake, age, hepatic and renal disease, and severe infection. Beware of the possibility of inducing hypoglycemia in patients taking the following:
- Ethanol
- Insulin
- Pentamidine
- Quinine
- Quinolones (Gatifloxin others rare)
- Sulfonylureas
Agents with lesser quality evidence as predisposing medications or illnesses were present:
- Ace Inhibitors (with diabetic agents)
- Propanolol ( less likely in other beta blockers)
- Trimethoprim/sulfamethoxazole (in renal compromise)
- Salicylates (high dose or intoxication)
Drugs induced hypoglycemia should always be considered in the differential diagnosis of every patient presenting with low blood glucose. Octreotide antagonizes pancreatic insulin secretion and should be considered for first-line therapy in the treatment of sulfonylurea-induced hypoglycemia particularly when glucose levels cannot be maintained by dextrose infusions. Octreotide is administered 50 mcg subcutaneously (1-10 mcg in children) every 12 hours.
Show References
Recently, there have been several news reports regarding the emergence of synthetic opioids in the U.S. and Canada. There are multiple synthetic opioids that have been identified as potential agents of abuse including W-18, U-47700, fentanyl derivatives, AH-7921 and MT-45. These compounds share a similar story with synthetic cannabinoid where they were synthesized for research purpose or by pharmaceutical companies but were not marketed. They are often sold as “research chemicals” over the internet.
In July 2016, three case reports have been published regarding several cases of U-47700 intoxication in San Diego, CA and Dallas, TX.
- Dallas, TX: A couple in their 20’s purchased U-47700 on the internet believing it to be “synthetic cocaine.” They both suffered CNS and respiratory depression after insufflation. Naloxone was not administered in both cases. The man was intubated while the woman was awake at time of presentation to the ED. U-47700 exposure was confirmed by liquid chromatography/tandem mass spectrometry.
- San Diego, CA: a 22 year old man with history of heroin abuse was found unresponsive and apneic (4 breaths per minute and pulse oximetry of 60%). He received naloxone 2 mg IV which completely reversed his CNS and respiratory depression. He admitted to purchasing U-47700 on the internet and its use prior to being found unresponsive. U-47700 exposure was confirmed using liquid chromatography/mass spectrometry.
- Central CA: 41 year old woman presented with CNS depression and pinpoint pupils after ingesting 3 tablets of “Norco” purchased from the street. Her intoxication was completely reversed with naloxone 0.4 mg IV and discharged after 4 hour observation. Fentanyl and U-47700 was detected in serum blood test.
It is unknown if currently available heroin is cut with above mentioned synthetic opioids. Like other opioid receptor agonists, administration of naloxone will likely reverse the opioid toxidrome. But clinical experience in reversing synthetic opioids intoxication with naloxone is limited.
Bottom line:
Irrespective of whether an ED patient is exposed to synthetic opioids or "traditional" opioids of abuse (prescription opioid pain medication or heroin), the management of opioid intoxication management remains unchanged for respiratory depression.
- Airway management: bag-valve assisted ventilation if needed
- Naloxone administration (initial dose: 0.04 to 0.4 mg IV) with titration as needed.
- naloxone's clinical duration of effect ranges from 30 to 90 minutes.
Show References
An Arbovirus is a virus transmitted primarily by an arthropod
- Comes from ARthropod-BOrne virus
- Arthropods include: mosquitos, ticks, sandflies
- Can have rare person-to-person transmission
- Blood borne
- Transfusion, sharing needles
- Organ transplantation
- Breast feeding
- Intrauterine
- Sexual transmission
- Blood borne
There are a number of major arbovirus families:
- Family Bunyaviridae
- Rift Valley, Crimean–Congo hemorrhagic
- Family Flaviviridae
- Dengue, West Nile, Zika, Yellow Fever
- Family Reoviridae
- Equine encephalosis
- Family Togaviridae
- Chikungunya, Western equine encephalitis
The main viral family that causes substantial human disease is the Flaviviridae family.
- Protection against mosquito bites is the best way to minimize risk for Flaviviridae infections if you are traveling in an area with these diseases.
Despite a lack of prospective data, end-tidal CO2 (ETCO2) is often proposed as a viable replacement for the traditional pulse check to identify return of spontaneous circulation (ROSC) in patients presenting to the Emergency Department in Cardiac Arrest. A recent study by Tat et al examined this very question. The authors prospectively enrolled 178 patients suffering out-of-hospital cardiac arrest (OHCA) and examined the accuracy of a rise in ETCO2 at predicting ROSC. The authors examined both a rise of 10 and 20 mm Hg in ETCO2. Of the 178 patients included in this cohort, 60 (34%) experienced ROSC. The sensitivity and specificity of ETCO2 to predict ROSC at a threshold of 10 mm Hg was 33% and 97% respectively. At a threshold of 20 mm Hg ETCO2 performed no better with a sensitivity and specificity of 20% and 99% respectively.
What this data suggests is while a rise of ETCO2 of greater than 10 is highly suggestive of ROSC, the contrary cannot be said. The absence of a spike in ETCO2 does not rule out ROSC, as the large majority of patients experiencing ROSC in this cohort did so without demonstrating a significant rise in ETCO2. This evidence suggests that ETCO2 is a poor surrogate for a pulse check.
Show References
The pediatric epiglottis is more "U" shaped, often overlies the glottic opening, and is "less in line with the trachea."1 Because of this, it has traditionally been taught that a Miller blade is the ideal laryngoscope.
Varghese et al compared the efficacy of the Macintosh blade and the Miller blade when placed in the vallecula of children between the ages of 1 and 24 months. The blades provided similar views and suffered similar failure rates. When the opposite blade was used as a backup, it had a similar success rate as the opposing blade.2 Passi et al also compared these two blades, this time placing the Miller blade over the epiglottis. Again, similar views were achieved.3
Show References
Show References
Predicting Fluid Responsiveness with ETCO2
- It is well known that almost 50% of critically ill patients do not respond to fluid resuscitaiton. For those that do not respond, indiscriminate fluid administration may be harmful.
- There is increasing emphasis on the use of dynamic markers of fluid responsiveness, namely passive leg raise (PLR), pulse pressure variation, respirophasic changes in the IVC, and many others.
- ETCO2 can also be used to assess fluid responsiveness in mechanically ventilated patients with no spontaneous respiratory effort.
- An increase in ETCO2 of at least 5% with a PLR has been shown to outperform arterial pulse pressure as a measure of fluid responsiveness.
Show References
30yo male weight lifter who 10 days ago had a painful left shoulder injury after bench press. The next morning his left anterior chest wall and left upper arm were bruised and swollen. He went to see his PCP who diagnosed him with a muscle strain. 8 days later the bruising and swelling have resolved but he still cant move his shoulder and comes to the ED.
http://321gomd.com/wp-content/uploads/2015/01/pec-major-tears.jpg
{kind=link}
The pec major attaches to the humerus and originates from the sternum and clavicle
Injury is usually due to tendon rupture off the humerus but can also occur at the muscle tendon junction or within the muscle belly itself.
Injury is becoming increasingly common due to the popularity in power lifting sports.
Mechanism: excessive tension on a maximally eccentrically contracted muscle.
Patients will complain of pain and weakness of the shoulder.
PE: Swelling and bruising to anterior medial arm. Palpable defect and deformity or anterior axially fold (may be hidden by swelling).
Weakness and pain with adduction and internal rotation and forward flexion
Chronic presentations can be challenging to diagnose. Consider ultrasound
Non operative treatment may be indicated for partial tears (sling, ice, NSAIDs)
Operative repair of tendon avulsions is very successful. Patients age, occupation/activity level and location of injury and condition of tear are considered.
- Emergency providers routinely care for neurologically injured patients, such as those with a SAH or TBI.
- Many of these patients will require airway management. In these patients, it is important to minimize any increase in ICP, as this can adversely effect cerebral perfusion pressure.
- When intubating the neurocritical care patient, consider a dose of fentanyl (2 to 5 mcg/kg) prior to intubation. This has been shown to decrease the sympathomimetic response to laryngoscopy.
Show References
-
Just the Facts:
-
112.5-million blood donations globally and half of these come from High-income countries
-
High-income countries more often use blood for supportive care during surgery, in traumas or therapy for malignancies
-
Low and middle-income countries more often use blood to manage pregnancy-related complications or in severe childhood anemia
-
General availability of blood is based on the donation rate
-
High-income countries have 33.1 donations/1000 people
-
Middle-income countries have 11.7 donations/1000 people
-
Low-income countries have 4.6 donations/1000 people
-
-
70 countries reported collecting fewer than 10 donations per 1000 people and half of these countries were in the African region
-
Disease prevalence in the region is reflected in the transmission rate of transfusion-transmissible infections (TTI)
-
Table 1. Prevalence of TTIs in blood donations (Median, Interquartile range (IQR)), by income groups
|
| HIV | HBV | HCV |
|
|---|---|---|---|---|
| High-income countries | 0.003% (0.001% – 0.040%) | 0.030% (0.008% – 0.180%) | 0.020% (0.003% – 0.160%) | |
| Middle-income countries | 0.120% (0.020% – 0.340%) | 0.910% (0.280% – 2.460%) | 0.320% (0.090% – 0.690%) | |
| Low-income countries | 1.080% (0.560% – 2.690%) | 3.700% (3.340% – 8.470%) | 1.030% (0.670% – 1.800%) |
Submitted by: Dr. Laura Diegelmann
Non-Musculoskeletal Causes of Neck Pain
Neck pain is a common complaint of people presenting to the ED. Most of the cases will be musculoskeleteal in origin and will respond to conservative therapy with NSAIDs or acetominophen. However, other non-musculoskeletal causes of pain could be lurky behind this benign complaint.
Don't forget to consider:
- Early mengingitis (84% of patients with meningitis will complain of neck stiffness)
- Myocardial infarction/angina. Women are known to have atypical symptoms and might just have dull pain in their neck. Be sure to ask about whether exertion increases the pain.
- Epidural Abscess- fever and neuro symptoms are often missing early on. Make sure to ask about risk factors for spinal epidural abscess.
- Vertebral Artery Discection - most common identifiable cause of stroke in your people. <50% are associated with trauma and <8% of patients have connective tissue disorder. Patients are at increased risk if they have had
- Cervical trauma (remember seen in < 50% of cases)
- Recent infection
- Hypertension
- h/o migraines
Although it is summer, preparations are being made for the 2016-2017 influenza season. The Center for Disease Control (CDC) no longer recommends the live attenuated influenza vaccine (LAIV4). The American Academy of Pediatrics has supported this statement.
The LAIV4 (the only intranasal vaccine available) was offered to patients over the age of 2 years without respiratory problems. Observational studies during the 2013-2015 seasons have shown that the LAIV4 has an adjusted vaccine efficacy of 3% compared to 63% for the inactivated vaccine (intramuscular). Children who received the intranasal vaccine were almost 4 times more likely to get the flu compared to children who received the injection.
Bottom line: Only the intramuscular shot is recommended for this upcoming season. This is causing many primary care practices to scramble to obtain enough vaccine.
Show References
- Endovascular intervention for acute ischemic stroke from ICA or proximal MCA occlusion is a Level IA recommendation1.
- Identification of patients who may benefit from endovascular intervention begins in the prehospital setting.
- Several prehospital stroke scales exist, but have not been validated using arterial imaging to determine the presence of LVOS.
- The Field Assessment Stroke Triage for Emergency Destination (FAST-ED) scale (see Table 1) was designed based on items of the NIH Stroke Scale (NIHSS) with higher predictive value for LVOS.
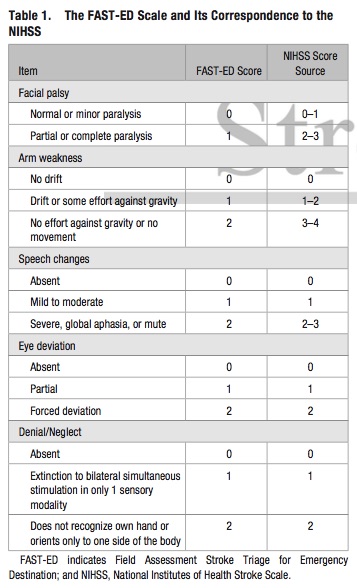
- The FAST-ED scale has comparable accuracy to predict LVOS to the NIHSS, and higher accuracy compared to the Rapid Arterial Occlusion Evaluation (RACE) and the Cincinnati Prehospital Stroke Severity (CPSS) scale
- The FAST-ED scale also provides 3 distinct groups for the likelihood of LVOS:
- Score 0 or 1: <15%
- Score 2 or 3: 30%
- Score >= 4: >60%
Bottom Line: Additional assessment of gaze deviation, aphasia and neglect, as included in the FAST-ED scale, increases the accuracy of predicting LVOS.