Search
Common herbs and supplements used to treat pain
1) Turmeric root - used for arthritis pain. Little evidence to support its use. May slow blood clotting/enhance anticoagulant/antiplatelet effects.
2) Boswellia - used for OA and RA pain. Little evidence to support its use.May interfere with anticoagulant drugs and leukotreine inhibitors.
3) St. John's Wort - used for HA, migraine, neuralgia, muscle pain, sciatica, fibromyalgia. Little to no evidence to support its use.May interfere with numerous medications including anticoagulants, digoxin and SZ medications.
4) Glucosamine and Chondroitin - used for OA, knee pain, back pain. The glucosamine/chondroitin arthritis intervention trial found that "the dietary supplements Glucosamine and Chondroitin, taken alone or in combination are generally ineffective for OA pain of the knee." May increase the effect of Warfarin.
5) KavaKava - used for HA, muscle pain. Insufficient evidence demonstrating effectiveness for treatment of painful conditions. May cause severe liver damage and potentiate drowsiness side effects of other medications.
6) Echinacea - used for pain, migraines, arthritis. Little evidence to support its use. May exacerbate symptoms of autoimmune disorders.
7) Valerian root – used for joint and muscle pain. Insufficient evidence to support its use. May potentiate sedative side effects of barbiturates and benzos.
8) Chinese Thunder God Vine – used for arthritis. There is some evidence to suggest that this agent has anti-inflammatory properties. Long term this agent may decrease bone mineral density in women, decrease fertility in men, and may produce GI side effects.
9) Feverfew – used for muscle pain, arthritis. Some evidence to suggest that may reduce frequency of migraine headaches. No evidence for benefit in RA. May enhance effects of anticoagulants and some drugs that undergo hepatic metabolism.
10) Cat’s claw – used for herpes zoster, bone pain, arthritis. Possible benefit for OA and RA in small studies in humans but no large study has shown benefit. May interact with clotting agents, BP meds and cyclosporine.
11) Black Cohosh – used for muscle pain and arthritis. Insufficient evidence demonstrating benefit. May be associated with severe liver side effects.
12) Bromelain – used for muscle pain, arthritis, knee pain. The NIH reports that bromelain may be effective for arthritis when used in combination with trypsin and rutin. May interact with amoxicillin and other antibiotics, anticoagulants and antiplatelet drugs.
13) Devil’s claw – used for muscle pain, back pain, arthritis, migraine. The NIH reports that “taking devil’s claw alone or with NSAIDs seems to help decrease OA related pain.” May increase effects of warfarin.
- diagnosis of exclusion
- bilateral leg pain only in the evening/night
- should NOT have a limp, pain, or symptoms during the day
- completely normal physical exam
- no systemic symptoms, localizing signs, joint involvement, or limitation of activity
- look for something else if there is anything wrong on review of systems, examination, or imaging studies
Show References
-
Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, previously named “anticonvulsant hypersensitivity syndrome,” is a severe adverse drug reaction which occurs in approximately 1 of every 1,000–10,000 uses of anticonvulsants.
-
Characterized by triad of fever, rash, and internal organ involvement.
-
Usually involves aromatic anticonvulsants such as phenytoin, carbamazepine, phenobarbital, primidone, lamotrigine, and possibly oxcarbazepine.
-
DRESS occurs most frequently within the first 2 months of therapy and is not related to dose or serum concentration.
-
Treatment includes prompt discontinuation of the offending agent. Patients should be admitted to the hospital and receive methylprednisolone 0.5–1 mg/kg/d divided in four doses. Other promising therapies include use of IVIG.
Show References
ECMO for ARDS and Refractory Hypoxemia
- Extracorporeal membrane oxygenation (ECMO), or extracorporeal life support (ECLS), is increasingly being used for a variety of cardiac and pulmonary conditions.
- Venovenous ECMO (VVE) should be considered in the treatment of patients with profound gas-exchange abnormalities that are refractory to accepted standards in ventilator management.
- Although indications vary slightly by institution, general indications for VVE include:
- Severe hypoxemia: PaO2/FiO2 < 80 despite high levels of PEEP for at least 6 hours
- Uncompensated hypercapnia with pH < 7.15
- Excessively high plateau pressures (> 45 cm H20)
Show References
Question
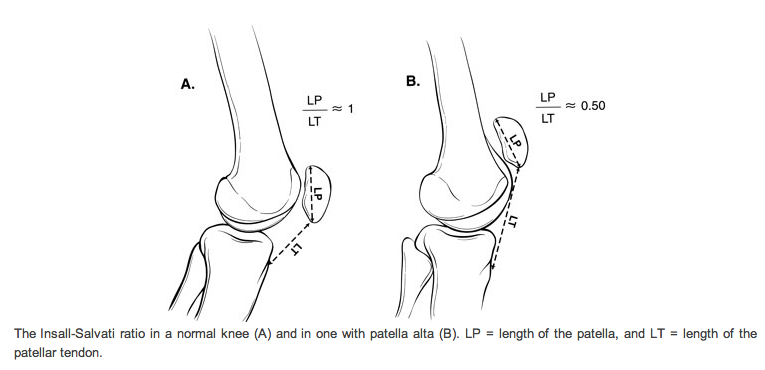
28 y.o. male felt his left knee "pop" after landing from a jump while playing basketball. Knee exam revealed limited knee extension. X-ray is shown. Diagnosis?

Show Answer
In the setting of critical drug shortages of ondansetron, prochlorperazine, and metoclopramide, consider droperidol as a viable option for the treatment of nausea and vomiting.
Although it is similar to haloperidol, it is actually FDA-approved for “prevention and/or treatment of nausea and vomiting from surgical and diagnostic procedures” (unlike haloperidol). Ironically, it is not approved for agitation, although it can be used for that indication.
Dosing for antiemesis is 1.25 to 2.5 mg IV/IM. Additional doses of 0.625 to 1.25 mg can be administered to achieve desired effect. Onset is 3-5 minutes and duration of effect is 2-4 hours. It should be administered via slow IV push over 2 minutes.
Why is it not commonly used? Black Box Warning for QTc prolongation. An ECG is a must prior to administration. Also be cautious in patients who are on other medications that can prolong the QT interval (www.qtdrugs.org).
- Antifungal agents (the -azoles)
- Class III antiarrhythmics
- Fluoroquinolones
- Low potency antipsychotic
Show References
AGE occurs when gas bubbles enter arteries or veins; AGE may cause clinical symptoms even with very small volumes of air.
Air enters the circulatory system via:
· Barotrauma – Alveolar injury allows air to enter systemic bloodstream; occurs in divers following rapid ascent after breath holding, during mechanical ventilation, chest tube placement, or bronchoscopy
· Decompression sickness – Dissolved gas precipitates out of bloodstream as bubbles; typically following scuba diving without appropriate time to ascend or prolonged flying in unpressurized aircrafts
· Direct injection of air into arterial or venous circulation – Examples include accidental IV injection of air, needle biopsy of lung, or aspiration of air during central line placement
Serious clinical manifestations include:
· Neurologic changes - loss of consciousness, confusion, or focal neurological deficits
· Hemodynamic changes – hypotension, arrhythmias, cardiac ischemia, or cardiac arrest.
· Respiratory changes – obstruction of pulmonary circulation, pulmonary edema, or hypoxemia
Treatment:
· Strict attention to ABC’s using high-flow O2.
· Keep head of bed elevated to minimize/reduce cerebral edema.
· Hyperbaric Oxygen (HBO) therapy is recommended for neurological manifestations or cardiovascular instability. Good outcomes associated with shorter intervals from air embolism to HBO. Typically only 1 to 2 treatments are needed; occasionally additional treatments are necessary.
Show References
Many physicians have the opportunity to invest in a variety of retirement funds. The most common commercial vehicle is a 401k. Academic and non-profits have access to an analogous 403b. Many physicians also have access to a 457b.
It is important to understand what it is, and most importantly how it differs from a conventional 401k or 403b. Like its' peers, it permit pre-tax contributions of a finite amount. They are offered through your employer and are bound to a specific vendor(s). These vendors provide a select number of investment choices specific to the employer contract. The maximum contribution for 2012 is $17,000.
The 457b is different from the other investment vehicles because of who and where your funds are held:
Non-governmental 457 plans have a number of restrictions that governmental ones do not. Money deferred into non-governmental 457 plans may not be rolled into any other type of tax-deferred retirement plan. It may be rolled only into another non-governmental 457 plan. Also, money deferred into non-governmental plans is not set aside in a trust for the exclusive benefit of the employee making the deferral. The Internal Revenue Code requires that money in a non-governmental 457 plan remains the property of the employer and is thus available to general creditors of the employer in legal or bankruptcy
If you work for a private entity, or a non-profit and they offer a non-governmental 457b, your personal funds are pooled with corporate resources. Your retirement contributions are at risk, should the company default and declare bankruptcy. This risk is apparently not born by GSRA 457b (Governmental agency 457b plans). A decade ago, this risk would seem insignificant. With the number of large companies and municipalities defaulting in this economic climate, prudence is warranted when considering this investment vehicle. DISCLAIMER - This pearl is not intended to provide financial advice. Please consult your HR department and / or financial advisor for additional information and advice.
Our old friend Captain Morgan (the rum pirate) may now be able to assist us during a shift, not just afterwards.
http://www.inquisitr.com/wp-content/2011/08/captain-morgans-pirate-ship-satisfaction-panama.jpg
In a small case series in last months Annals of Emergency Medicine, a new reduction maneuver was described as an alternative to the traditional Aliis's maneuver.
The maneuver is named after the pirate spokesperson for the similarities in body positioning.
The patient is placed supine on a stretcher. The pelvis is fixed to a backboard with a strap. The patient's hip and knee are flexed to 90 degrees. The physician places one foot on the back board with the same knee behind the patient's knee. By holding the patient's ankle down, the patient's knee is kept in flexion. The physician then lifts his/her calf, thereby applying an upward force to the hip while gently rotating the lower leg from side to side.
http://www.youtube.com/watch?v=l07K-mO2X84
with a slight variation
http://www.youtube.com/watch?v=sGQZaqB48rw
The success rate was 12 of 13 cases. The single failure occurred in a patient with an acetabular fracture with an intra-articular fragment requiring open reduction. There were no described neurovascular complications or injuries to the knee. The technique limits the physician's risk of back strain and of falling from the stretcher.
Show References
Potential Causes of Neonatal Apnea and Bradycardia
• Central nervous system
Intraventricular hemorrhage, drugs maternal/fetal, seizures, hypoxic injury, herniation, neuromuscular disorders, brainstem infarction or anomalies (e.g., olivopontocerebellar atrophy), general anesthesia.
• Respiratory
Pneumonia, obstructive airway lesions, upper airway collapse, atelectasis, extreme prematurity (<1,000 g), phrenic nerve paralysis, severe hyaline membrane disease, pneumothorax, hypoxia, malformations of the chest.
• Infectious
Sepsis, meningitis (bacterial, fungal, viral), RSV
• Metabolic
Hypoglycemia, hyper/hyponatrmia, hyperammonemia, decreased organic acids, hypothermia.
• Cardiovascular
Hypotension/hypovolemia, heart failure, PDA, anemia, vagal tone.
As we go through the problems of national drug shortages it is important to remember the old drugs but to also remember why they became old and seldom used drugs. Prime example is many hospitals are beginning to develop shortages of rocuronium - the nondepolarizing paralytic that has a fast onset. This shortage has caused many to switch back to succinylcholine. The following case report should serve as reminder of how succinylcholine - due to its depolarizing nature and fasciculations - can cause a transient but significant hyperkalemia.
Succinylcholine-induced Hyperkalemia in a Patient with Multiple Sclerosis
The Journal of Emergency Medicine, 12/13/2011
Levine M et al. – This case report describes a 38–year–old woman with multiple sclerosis who developed life–threatening hyperkalemia after the administration of succinylcholine during rapid sequence intubation. This case highlights the potential for iatrogenic hyperkalemia after succinylcholine in patients with neurologic diseases, including multiple sclerosis.
SAH and Pulmonary Edema - Think Twice About Diuresis!
- Delayed cerebral ischemia (DCI) is the most common cause of secondary neurologic injury in patients with aneurysmal subarachnoid hemorrhage (SAH).
- Intravascular volume depletion is one of several factors thought to cause, or worsen, DCI.
- Pulmonary edema frequently occurs in patients with SAH.
- A recent study in patients with SAH and pulmonary edema demonstrated that many were not volume overloaded. In fact, many were intravascularly volume depleted.
- Think twice about aggressive diuresis in patients with SAH and pulmonary edema, as this may exacerbate volume depletion and may worsen DCI.
Show References
Question
20 year old female complains of “itchy” rash to her foot x 1 week and recently the rash has spread to her other other foot and both hands (shown below). No past medical history, no fever or chills, no mucus membranes involvement, no new medications, no tick bites, no travel. She is also 16 weeks pregnant. What’s the diagnosis?

Show Answer
Show References
The WBC count is normal in up to 45% of elderly patients with bacteremia. The most predictive factors for bacteremia in the elderly are delirium, vomiting, bandemia, and tachypnea.
Show References
Flexor Tenosynovitis
- This is a rapidly spreading infection of the finger and hand.
- Often starts as an infection in the finger that then spreads into the hand due to the flexor sheaths.
- The flexor tendon sheaths of the long, index, and ring finger extend from the distal phalanx to the superficial palmar arch, and some even extend to the wrist.
- Most patient will need to be admitted for IV antibiotics and a hand consult for probable operative I&D
- You can diagnosis flexor tenosynovitis by documenting the four Kanavel signs:
- Fusiform swelling of the finger
- Finger held in partial flexion (position of comfort)
- Percussion tenderness along the flexor tendon
- Increased pain with passive extension of the finger
You can follow this link, http://www.youtube.com/watch?v=qf9SW0ChsCU , to see the physical exam findings of flexor tenosynovitis
Never be the first or last person to use a drug
Vioxx was once touted to be the drug that would be the new standard for anti-inflammatories until it was found to increase your chance of MI by 33% and cause hypertension.
Dabigatran was recently pulled from Japan markets and now is dealing with an impressive meta-analysis by Uchino et al. It showed that dabigatran was significantly associated with higher risk of MI or ACS than other agents.
Control arms (included warfarin, enoxaparin or placebo): MI rate 83 per 10,514
Dabigatran arms: MI rate 237 per 20,000
OR 1.33; 95% CI, 1.03-1.71; p=0.03
The rush for what is perceived as a panaceae for all that is wrong with coumadin could actually cause an MI while it tries to prevent a stroke in nonvalvular a-fib.
Look at the study and decide for yourself and remember Vioxx:
http://archinte.ama-assn.org/cgi/content/full/archinternmed.2011.1666v1
Fungal endopthalmitis is an intraocular infection of the aqueous and/or vitreous humor secondary to fungal pathogens; Candida and Aspergillus species are the most common pathogens.
Risk factors: intravenous drug abuse (#1 risk factor), critical illness, systemic fungal infection, immunosuppression (from cancer or medications), diabetes, and alcoholism.
Have a high-index of suspicion for endopthalmitis when patients with systemic fungal disease have visual symptoms; endopthalmitis is present in up to 33% of patients with systemic fungal disease.
Symptoms include:
- Visual disturbances / visual loss
- Eye pain
- Photophobia
- Red eye
- “Floaters”
- Asymptomatic
Inspection of both the anterior and posterior chamber is essential to during evaluation; several small yellow-white circular or “fluffy” lesions with surrounding hemorrhage are demonstrated.
Definitive diagnosis made by vitreous biopsy, culture, or PCR; presumptive treatment is acceptable if systemic fungal disease has been demonstrated.
Treatment with Amphotericin B or Voriconazole may be used for broad-spectrum fungal coverage until specific culture and sensitivities return.
Show References
As many as 1/3 of patients with proven ACS have no chest pain at presentation. Among the more common alternative presentations (anginal equivalents) are dyspnea, diaphoresis, nausea/vomiting, and syncope/near-syncope.
Note also that the absence of pain does not confer a better prognosis. The overall in-hospital mortality rate for patients with painless presentations is 13% vs. 4.3% for patients with chest pain.