Search
Pacing Atrioventricular Block
- Atrioventricular (AV) block is classically treated with restoration of heart rate via right ventricular pacing, however high rates of right ventricular pacing is associated w/ left ventricular systolic dysfunction
- A recent multi-center randomized control trial (RCT) assessed the efficacy of right vs biventricular pacing in heart failure w/ AV block [BLOCK HF Trial]
- Primary outcomes of: morbidity, mortality, and adverse left ventricular remodeling were shown to be significantly lower in biventricular vs right ventricular pacing
- In patients with a high rate of pacing and/or an abnormally low left ventricular ejection fraction biventricular pacing may be more advantageous than conventional right ventricular pacing
Show References
Post Operative Fever is extremely common, and with the increase in same day surgery this is a common complaint presenting to the ED. The mnemonic "5Ws" are often taught to remember the causes. They are:
- Wind - Pneumonia, aspiration, pulmonary embolism, and atelectasis
- Water - urinary tract infection
- Walking - Deep Venous Thrombosis or pulmonary embolism
- Wound - surgical wound infection
- Wonder drugs - Drug fever, or infection due to indwelling lines, or a reaction to blood products
Though many surgical textbooks report that atelectasis is the most common cause of early post-operative fever, some even claiming that it is responsible for over 90% of febrile episodes in the first 48 hours after surgery; a recent review in CHEST (reference below) showed that there is no evidence to support this. We often see atelectasis in medical patients too, and few if any of them have fever. The CHEST review found that there was no clear evidence that atelectasis causes fever at all.
Pearl: Temperature >38.9C should raise concern for a true infection, where lower temperatures can be due to pulmonary embolism, DVT, drug fever, etc….
Show References
Show References
General Information:
The H’s and N’s refer to hemagglutinin and neuraminidase—two proteins on the surface of the Influenza A virus that help it attach. Here’s a quick breakdown of important emerging strains of influenza:
Avian flu:
- H5N1 (aka. Highly Pathogenic Avian Influenza A): Case Fatality Rate (CFR) 60%, no sustained person to person transmission, primarily in Asia and Middle East--first death in the Americas occurred in Canada last week (returned traveller from China)
- H7N9: new strain of avian influenza identified this year, 135 cases so far, CFR 33%, no sustained person to person transmission, found in China
Swine flu:
- H1N1: pandemic flu of 2009 making a comeback. causes more severe disease in young and middle-aged adults, predominant this season in the US (of subtyped virus tests ~98% were H1N1)
Relevance to the EM Physician:
As the frontline against the flu virus, we should know what to expect. H1N1 has predominated this flu season—so far 60% of hospitalizations occurred in patients aged 18-64, which is unusual. H7N9 is new on the scene but might be imported, and H5N1 has arrived.
Bottom Line:
Expect to see more severe illness in the 18-64 y/o age group due to H1N1. Watch for more deadly flu imports--obtain a travel history and notify the CDC of severe influenza-like illness in returned travellers.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Show References
Determination of Brain Death
- With the recent media spotlight on brain death (irreversible end of brain activity) due to a few recent cases, it would be helpful to review the definition.
- Rule out alternative causes including hypothermia, drug-induced coma, metabolic abnormalities, or severe electrolyte disturbances.
- A clear irreversible cause must be known based on history and diagnostic studies.
Clinical Examination
- Patient should be unresponsive to verbal or noxious stimulation, with the exception of spinally mediated responses.
- Absence of brainstem Reflexes
- No pupillary response
- Absent corneal reflex
- Absent gag and cough reflex
- Absent cervico-ocular reflex (Doll’s Eyes Maneuver)
- Absent vestibulo-ocular reflex (Cold Calorics)
- Apnea Testing (disconnecting the ventilator and evaluating respiratory drive)
If apnea testing cannot be performed due to instability, hypoxia, or cardiac arrhythmias, then a confirmatory test should be performed (from highest to lowest sensitivity):
- Angiography (lack of intracranial flow)
- EEG
- Transcranial Doppler
- Technetium-99 brain scan
- Somatosensory evoked potentials
There is state to state variation on who can perform the test and how many separate examinations need to be performed before brain death can be legally declared.
For a great review on some of the pitfalls in making the diagnosis and difficulties with the examination, please see the attached article.
Show References
Attachments
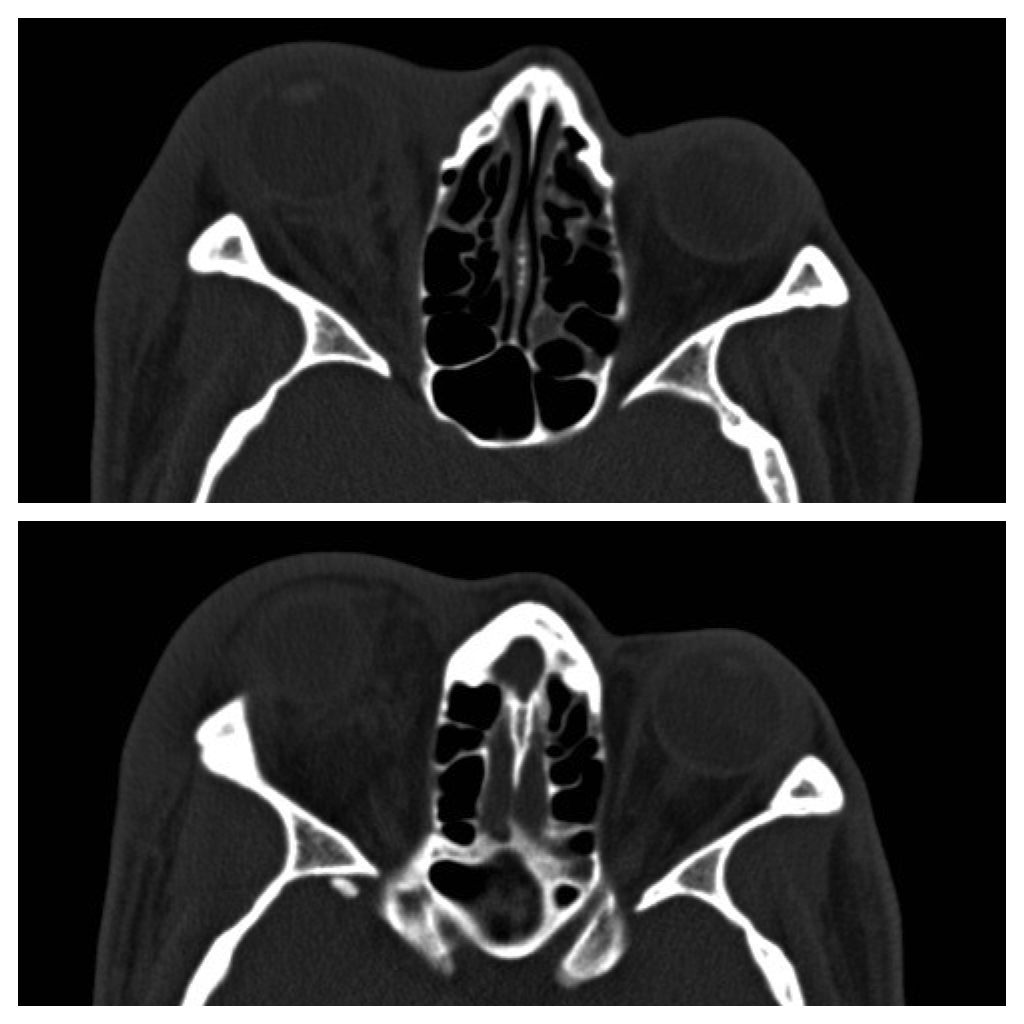
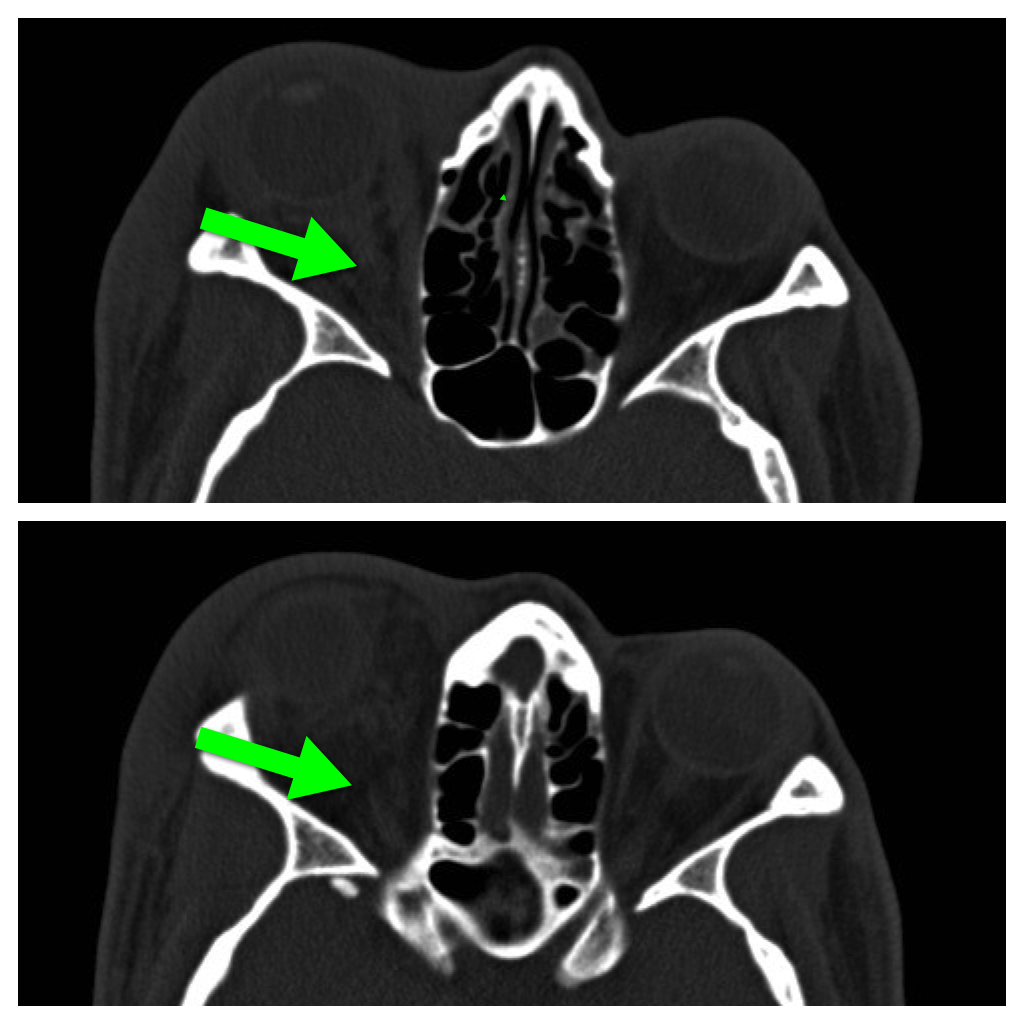
Question
42 year-old male s/p assault complains of right sided facial pain, swelling, and decreased vision. Physical exam reveals subconjunctival hemorrhage, proptosis, afferent pupillary defect, and a firm globe. What's the diagnosis and what's the emergent treatment?
Show Answer
Show References
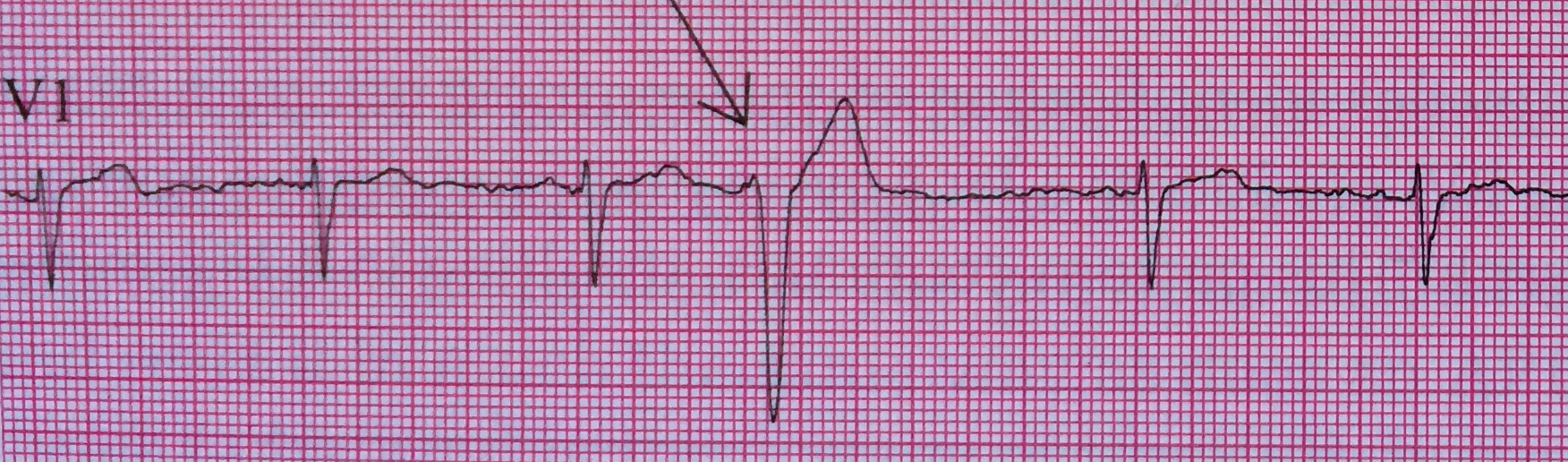
Differentiation between right and left ventricular origin of premature beats can be useful clinically.
-
PVCs arising from the right ventricle have a left bundle branch block morphology (dominant S wave in V1)
-
PVCs arising from the left ventricle have a right bundle branch block morphology (dominant R wave in V1)
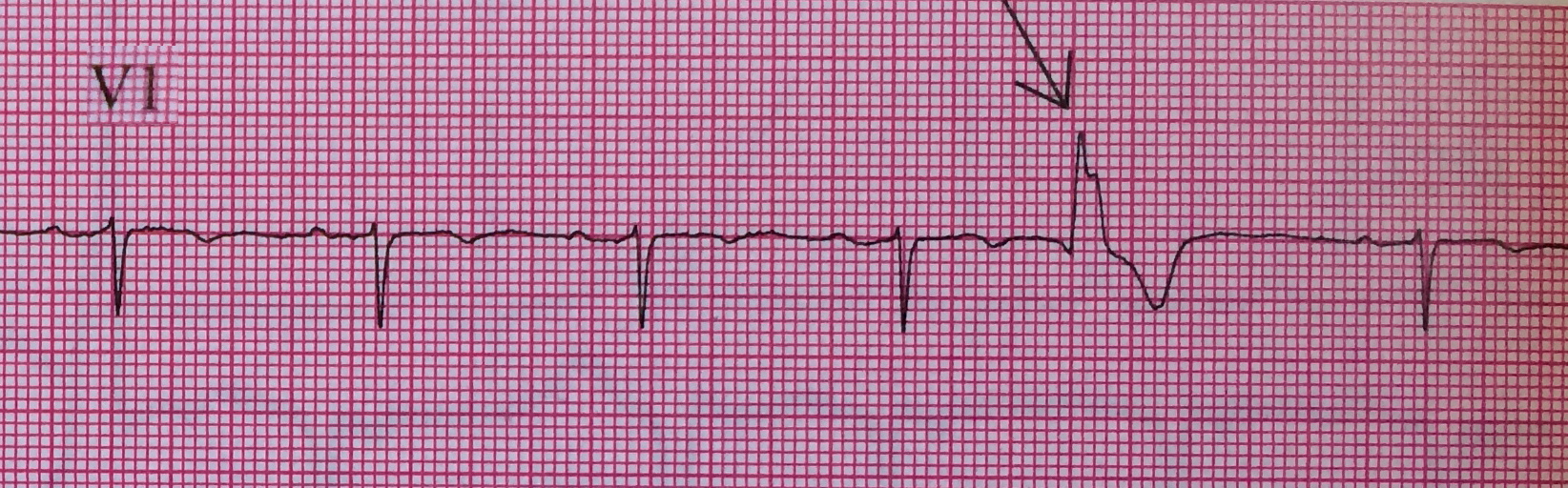
Left Ventricular premature beats are more often associated with heart disease and may precipitate ventricular fibrillation, whereas right ventricular premature beats are commonly seen in individuals with normal hearts.
Want more emergency cardiology pearls? Follow me @alifarzadmd
Show References
Show References
Current evidence does not support the use of fasciotomy or dermotomy following North American Crotalinae envenomation with elevated intracompartmental pressures. [1]
A new case report of a 17-month old bitten by a copperhead snake reinforces that early and adequate administration of crotaline Fab antivenin is the treatment of choice. [2]
Many experts recommend against measuring compartement pressures altogether; we know it will be elevated.
Show References
Background Information:
Infections by Staphylococcus aureus cause significant morbidity and mortality around the world, but up until now no effective vaccines have been developed. Some prior attempts at vaccination actually led to higher mortality in the vaccinated group. However, a group at University of Iowa developed a vaccine targeting S. aureus virulence factors that has shown promise in animal models.
Pertinent Study Design and Conclusions:
- Rabbits (often used as an analog for human S. aureus disease) were inoculated with the vaccine.
- Each rabbit then had a high dose of various strains of MSSA or MRSA introduced via the respiratory tract and were monitored for pneumonia.
- 86/88 vaccinated rabbits survived while only 1/88 non-vaccinated rabbits survived.
Bottom Line:
While not available for human use yet, this is the first promising vaccine against S. aureus infections (including MRSA). Stay tuned…
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Show References
- If less than 24 hours since injury, consider diagnostic angiography and intra-arterial TPA, and heparin infusion, Prostacyclin infusion.
- Angiography and Bone Scan can be used to prognosticate clinical course.
- Consider Hyperbaric Oxygen Therapy for moderate to severe frostbite- multiple case reports of significant improvement with HBOT even if delayed by several days.
Show References
Pearls for the Crashing LVAD Patient
- Left ventricular assist devices (LVAD) are placed as a bridge to transplant, bridge to recovery, or as destination therapy.
- As thousands of LVADs have been implanted, it is likely that a sick LVAD patient will show up in your ED or ICU.
- In addition to pump thrombosis (UMEM pearl 12/31/13), two complications to also consider in the crashing LVAD patient include infection and arrhythmias.
- Infection:
- The driveline and pump pocket are the most common locations for device infection.
- Most are caused by Staphylococcus and Enterococcus organisms.
- For pump pocket and deeper wound infections be sure to also add coverage against Pseudomonas species.
- Arryhthmias:
- The highest incidence is within the first month after implantation.
- Consider a "suction event," where the inflow cannula contacts the ventricular septum.
- Suction events can be caused by hypovolemia, small ventricular size, or RV failure and are treated with fluid resuscitation and decreasing the LVAD speed.
Show References
Question
37 year-old male presents after sustaining a burn from a pot of boiling water. He states that his skin started to blister a few hours after and it’s quite painful. What type of burn does he likely have?

Show Answer

Show References
Head lice infestation is a common problem in the United States with treatment costs estimated at 1 billion dollars and cases affecting millions of children each year. Many of these children present to the ED for care...lucky us! Traditional therapies containing permethrin and pyrethrins are having increased rates of treatment failure likely secondary to increasing resistance and medication noncompliance. The typical first line agents require multiple doses. There are safety concerns regarding therapies that contain malathion and lindane in children. Is there another option? Topical ivermectin 0.5% lotion applied to scalp in a single dose has been shown to be effective and safe for treatment of head lice infestation in children older than 6 months. It was FDA approved at the end of 2012. Considerations include cost. Sklice lotion is expensive!
The NEJM article was considered an "editors pick" by the AAP as one of the best articles of 2012-2013.
Show References
Assessment of Intermediate Coronary Lesions
- Coronary angiography alone to assess CAD is fraught with subjectivity
- Fractional flow reserve (FFR) has become the standard to assess/quantify obstructive CAD; it determines the myocardial flow in the presence of stenosis identifying the lesion responsible for ischemia
- FFR assesses focal stenosis, but does not consider diffuse atherosclerotic narrowing or microcirculatory dysfunction as contributors of ischemic heart disease
- An index of microcirculatory resistance (IMR) can be concomitantly measured with FFR during cardiac catheterization to specifically evaluate the microvasculature
- Coronary flow reserve (CFR) was the 1st proposed method for assessment of intermediate coronary lesion, but proved suboptimal because of its variability especially in patients with microvascular dysfunction (diabetes, prior MI, etc.)
- Utilization of FFR, IMR, and CFR together support the existence of differentiated patterns of ischemic heart disease & may help to determine future ischemic events
Show References
46 patients treated with high-dose droperidol (10-40 mg) were studied prospectively with continuous holter recording.
What they did
Patients initially received 10 mg droperidol as part of a standardized sedation protocol (for aggression). An additional 10 mg dose was given after 15 min if required and further doses at the clinical toxicologist's discretion.
Continuous 12-lead holter recordings were obtained for 2-24 hours. QTc > 500 msec was defined as abnormal (with heart rate correction - QTcF).
What they found
Only 4 patients had abnormal QT measurements, three given 10 mg and one 20 mg. All 4 had other reasons for QT prolongation. No patient given > 30 mg had a prolonged QT. There were no dysrhythmias.
What it means
There was little evidence supporting droperidol being the cause and QT prolongation was more likely due to pre-existing conditions or other drugs.
Show References
Tranexamic acid (TXA) is an antifibrinolytic that prevents clot breakdown by inhibiting plasminogen activation and plasmin activity
The CRASH-2 trial enrolled 20,211 adult trauma patients with significant hemorrhage (SBP <90 or HR 110) or at significant risk of hemorrhage
Patients were randomized to 1 gram TXA over 10 minutes followed by an infusion of 1 gm over 8 hours vs placebo
There was a significant reduction in the relative risk off all cause mortality of 9% (14.5% vs 16%, RR 0.91, CI 0.85-0.97, p = 0.0035)
The patients that benefited most were those most severely injured, and in those treated in less than 3 hours of injury.
Show References
Background Information: While the concept of Emergency Medicine is fairly well understood in the United States, it is less clear in countries where the concept is not as well established. This has caused quite a bit of confusion and hindered progress and collaboration.
Pertinent Study Design and Conclusions: In a recent consensus conference held at SAEM several definitions were standardized.
- Acute Care: all promotional, preventive, curative, rehabilitative, and palliative actions, whether oriented toward individuals or populations, whose primary purpose is to improve health and whose effectiveness depends largely on time-sensitive and frequently rapid intervention.
- Emergency Medicine: a named field of specialty practice for which formal training prepares a candidate whose competence is officially standardized and regulated (thus EM is a subset of acute care)
- Emergency services: the sum of all efforts to deliver effective health action in response to extreme risk under intense time pressure
- Emergency care: the subset of emergency services focused on delivery of curative interventions targeting severe clinical cases
Bottom Line:
It is imperative that the same terminology be used when discussing the delivery of care on a time-sensitive basis.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Show References
VAD thrombosis: A Must Know VAD Complication
The HeartMate left ventricular assist device (LVAD) is one of the most frequently placed LVADs today. Originally, it was thought to have a lower incidence of thrombosis due to its mechanical design. However, a recent multi-center study published in the NEJM reported a dramatic increase in the rate of thrombosis since 2011 in the HeartMate II device. The report found:
-
An increase in pump thrombosis at 3 months after implantation from 2.2% to 8.4%
-
The median time from implantation to thrombosis was 18.6 months prior to March 2011, to 2.7 months after.
Pump thrombosis is a major cause of morbidity and mortality (up to almost 50%!!) and is a can't miss diagnosis. It's important to keep thrombosis on the differential for any VAD patient presenting with:
-
Power spikes or low pump flow alarms on the patient's control box
-
Pump (VAD) failure
-
Recurrent/new heart failure
-
Altered mental status
-
Hypotension (MAP < 65)
-
Signs of peripheral emboli (including acute CVA)
Useful lab findings suggestive of thrombosis include:
-
Evidence of hemolysis
-
LDH > 1,500 mg/dL or 2.5-3 times the upper limit of normal
-
Hemoglobinuria
-
Elevated plasma free hemoglobin
Bottom Line: In the patient with suspected VAD thrombosis, it is important to contact the patient's VAD team immediately (CT surgeon, VAD coordinator/nurse, VAD engineer). Treatment should begin with a continuous infusion of unfractionated heparin, while other treatment options can be discussed with the VAD team.
Show References
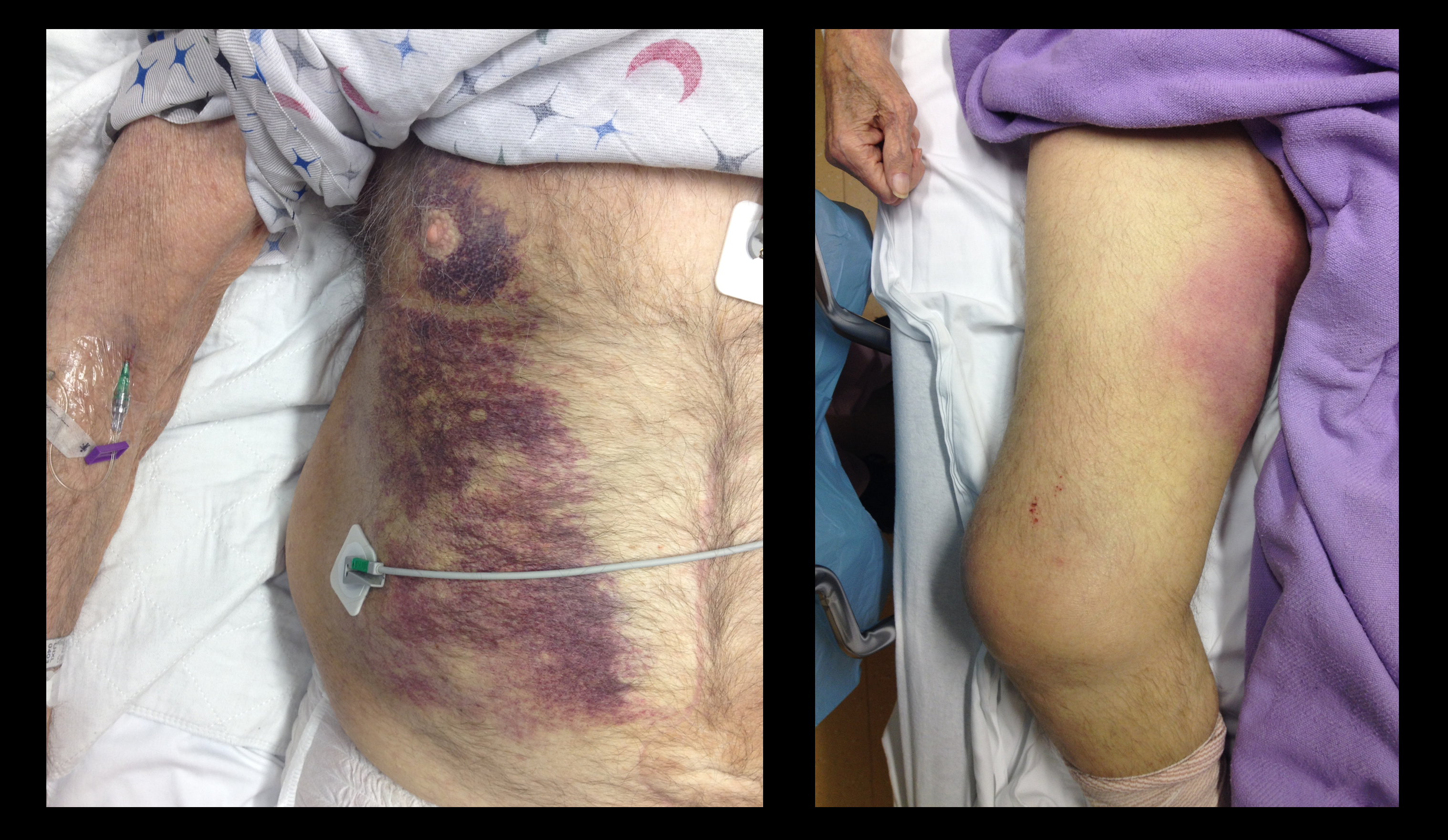
Question
68 year-old male presents with weakness after surgical repair of his abdominal aorta. What’s the diagnosis and name at least one eponym for the signs displayed (there are five total)?