Search
Peritoneal dialysis (PD) is a commonly used form of dialysis for pediatric patients with end-stage renal disease, particularly in children less than five years of age.
One well known complication to this mode of dialysis is PD-associated peritonitis.
Children may present with fever, abdominal pain and a cloudy dialysate.
If peritonitis is suspected, obtain sample of dialysate fluid and send for cell count, Gram’s stain and culture.
Cell count in PD-associated peritonitis is usually WBC >100 with >50% neutrophils.
Both gram-positive and gram-negative organisms are involved with PD-associated peritonitis . Keep both MRSA and Pseudomonas in mind.
In the ED, empiric therapy should cover both gram-positive and gram-negative organisms. Initiate antibiotic therapy with vancomycin and either a third-generation cephalosporin (ceftazidime) or aminoglycoside, respectively.
For PD-associated peritonitis, intraperitoneal (IP) administration of antibiotics is preferred over IV.
Show References
There are an increasing number of intranasal medications commercially available for use, which is opportune as more and more intravenous medications become scarce.
These now include:
| Generic name | Brand Name | Usage |
| Fentanyl | Instanyl | Opiate analgesic |
| Ketorolac | Sprix | NSAID analgesic |
| Desmopressin (DDAVP) | Stimate | Bleeding |
| Vitamin B12 | Nasobal | Anti-migraine (yes!) |
| Sumatriptan | Imitrex | Anti-migraine |
| Zolmitripran | Zomig | Anti-migraine |
*******In addition, you can administer glucagon, midazolam and narcan intranasally as well.
Show References
- In patients presenting with bilateral miosis (i.e. pinpoint pupils) of unknown etiology, the astute clinician may consider acute pontine injury, opiate overdose, or medication-related causes as the source.
- In such cases, one should consider performing the simple corneal reflex test to evaluate mid and lower pontine function.
- This test consists of lightly touching the cornea with the cotton swab of a Q-tip and observing blink responses in both eyes. It assesses afferent fifth nerve (sensory) and efferent seventh nerve (motor) function.
- A normal response is simultaneous (i.e. consensual) eye blinking. An abnormal response may be manifest by midline deviation, followed by relaxation, of the lower eyelids.
- TAKE HOME POINT: Corneal reflex testing is an easy way to help distinguish pontine injury from an opiate overdose in patients presenting with pinpoint pupils. Confirmatory studies by way of brain imaging should follow.
Fever and ICH
- Fever is a common event in patients with intracerebral hemorrhage (ICH) and is associated with an increased length of ICU stay, cognitive impairment, and poor outcome.
- While much of the management (and controversies) of the patient with ICH focuses on blood pressure control and reversal of oral anticoagulants or antiplatelet agents, don't forget about temperature control.
- Aggressively treat temperatures ≥ 38.3oC in patients with an ICH.
- Importantly, there is currently insufficient evidence to support a superior method of fever control (antipyretics or surface/intravascular cooling devices).
Show References
Question
Question: 50-year-old diabetic female s/p foot burn several weeks ago, now presenting with pain and discharge from a poorly healing wound. Diagnosis?

Show Answer
Hostile behavior appears to be a predictor of ischemic heart disease and myocardial infarction. Prior studies have demonstrated this association, and now one more study has supported this. In short, researchers from Nova Scotia demonstrated that observed hostility was a predictor of ischemic heart disease and myocardial infarction (2-fold), independent of age, sex, Framingham Risk Score, and other psychosocial risk factors.
The key takeaway point of this fun, but validated concept, is that in addition to exercising and eating right, we all just need to relax a bit more. And the next time you have to deal with an angry consultant, just tell him to chill out or he'll die!
Show References
An acute increase in the INR over 3 in patients with chronic kidney disease (CKD) is often associated with an unexplained acute increase in serum creatinine and an accelerated progression of CKD.
Kidney biopsy in a subset of these patients showed obstruction of the renal tubule by red blood cell casts, and this appears to be the dominant mechanism of the acute kidney injury. This has been termed warfarin-related nephropathy (WRN).
In 15,258 patients who initiated warfarin therapy during a 5-year period, 4006 had an INR over 3 and creatinine measured at the same time. A presumptive diagnosis of WRN was made if the creatinine increased by over 0.3 mg/dl within 1 week after the INR exceeded 3 with no record of hemorrhage. WRN occurred in 20.5% of the entire cohort, 33.0% of the CKD cohort, and 16.5% of the no-CKD cohort. Other risk factors included age, diabetes mellitus, hypertension, and cardiovascular disease. The 1-year mortality was 31.1% in patients with WRN compared with 18.9% in those without WRN, an increased risk of 65%.
Take home message: Although the mechanisms are not clear, be very wary of even a small creatinine bump in patients presenting with an INR > 3 on warfarin therapy. Yet another reason to fear warfarin...
Show References
You are seeing a high school football player following a head injury. After your exam or head CT, you determine the child to have had a mild traumatic brain injury (aka concussion). You are ready to discharge him home when the parents or coach ask you when he can return to playing football.
A concussion is a form of functional, rather than structural, brain injury that displays no evidence of injury on structural neuroimaging. Symptoms include transient loss of consciousness, amnesia, vomiting, headache, poor school work, sleep changes, and emotional lability. Remember that children’s brains (even adolescents) are still developing, and are more prone to prolonged recovery following injury.
Recovery of symptoms usually follows a sequential course. Current guidelines recommend a stepwise return to play (aka concussion rehabilitation) involving both physical and cognitive rest (e.g. no texting, video games, limited school work). Once asymptomatic, the patient goes through each stage with at least 24 hours between stages. If symptoms return during a stage, then the patient is expected to return to the previous stage for 24 hours before attempting the higher stage again.
Return to Play Guidelines:
| Rehabilitation stage | Functional Exercise |
| Complete physical and cognitive rest |
| Walking, swimming, stationary cycling at 70% maximal heart rate, no resistance exercise |
| Specific sport related drills but no head impact |
| More complex drills, may start light resistance training |
| After medical clearance, participate in normal training |
| Normal game play |
References:
- Halstead ME, Walter KD, and The Council on Sports Medicine and Fitness. Pediatrics. 2010;126:597-615.
A growing trend in EDs is to have a dedicated ED Pharmacist present to assist with the evaluation of a patient's medication list, appropriate and safe drug administration and to improve drug delivery times. To date, it has been difficult for hospitals to determine if this was a cost-effective measure. There has been increasing research that has shown the proven benefits that physicians feel when they have an ED Pharmacist. With the aging population, increasing polypharmacy, core measure and national patient safety goals all rising to the top of hospital initiatives, the ED pharmacist will be proven to be a valuable cog of the ED - as UofMd already knows
1) Improved safety - this study showed an ED pharmacist caught 2.9 errors/100 medications, very important considering the cost of just one severe reaction can cause a hospitalization or even litigation(1)
2) Improved time to delivery of medication - this study showed improved time of delivery of medications not found in a Pyxis from 61 min with no pharmacist decreased to 47 min with ED pharmacist.(2)
Further studies will be needed to determine the true cost:benefit however with core measures like 6hr time to administration of antibiotics and the safe/timely adminstration of tPA combined with patient safety/quality goals - the value of an ED pharmacist will only be accentuated.
Show References
- Marcus Gunn Pupil is a highly objective and significant clinical manifestation of a relative afferent pupillary defect (RAPD), indicating decreased pupillary response.
- The "swinging flashlight test" whereby a light is shone alternately back and forth between both eyes, can be used to elicit this finding. A normal response results in constriction of both pupils, which indicates intact direct and consensual pupillary light reflex. An abnormal response due to RAPD, however, results in minimal constriction of both pupils when the light in shone in the affected eye, causing one to perceive the presence of pupillary dilation.
- See the attached image which contrasts a normal response (top) to an abnormal response (bottom).
- Marcus Gunn Pupil is most commonly associated with lesions at the level of the optic nerve (proximal to the optic chiasm) or severe retinal disease. Associated conditions include severe glaucoma, optic nerve tumors, and ocular trauma.
Attachments
· The use of epinephrine in cardiac arrest is currently standard of care.
· Several observational and non-randomized trials have demonstrated the efficacy of epinephrine in cardiac arrest, but there has never been a randomized double-blind placebo-controlled trial in humans.
· A recently published Australian trial randomized cardiac patients (of any type) to receive either 1 mg of epinephrine (n=272) or 0.9% normal saline (n=262); the primary end-point was survival to hospital discharge. Secondary end-points were pre-hospital return of spontaneous circulation (ROSC) and neurological outcomes at hospital discharge.
· Significantly more patients had pre-hospital ROSC in the epinephrine group (regardless of the underlying rhythm), however, there was no statistically significant difference in survival to discharge (the primary outcome) between groups.
· This randomized double-blinded placebo-controlled trial raises many new and interesting questions about epinephrine, but more study is needed before changing current practice.
Show References
Elderly patients in general have a lower baseline body temperature than younger patients. Consequently, it makes sense to redefine the definition of what constitutes a "fever" in the elderly. Rather than using the typical oral temperature cutoff of 38o C (100.4o F) for defining a fever, instead consider using 37.2o C (99o F). Redefining fever in this way increases the sensitivity for detecting bacterial infections from 40% to 83% while retaining an 89% specificity.
Show References
Saturday night palsy - radial nerve mononeuropathy due to improper arm positioning associated with inebriated sleep.
Physical examination - Wrist and finger drop.
Patients may have findings suggestive of ulnar nerve co-involvement (interossei testing) which may falsely lead the examiner to consider a more proximal location for the lesion such as the brachial plexus.
The finger drop caused by the radial nerve lesion places the hand at a mechanical disadvantage. Adjust for this by examining the hand on a flat surface (stretcher, counter top). With the fingers now supported in extension at the MCP joint (no longer "dropped"), the interossei can now be tested in isolation and will be normal.
- The Glascow Coma Scale (GCS) was originally derived from data from adult head injuries; its use is therefore not always applicable or reliable in non-traumatic cases (particularly those which are complex) or children under a certain age.
- Scoring Range = 3 to 15.
- Severe is less than 9.
- Scores of 8 or less should prompt strong consideration for airway management via intubation.
- The motor score is the most predictive and clinically useful component.
- See GCS Score below:
EYE OPENING
4 = spontaneous
3 = to voice
2 = to pain
1 = none
VERBAL RESPONSE
5 = orientated
4 = confused
3 = inappropriate
2 = incomprehensible
1 = none
MOTOR RESPONSE
6 = obeys command
5 = localizes pain
4 = withdraw to pain
3 = decorticate
2 = decerebrate
1 = none
Spontaneous Bacterial Peritonitis
- Critically ill patients with end-stage liver disease (ESLD) may be some of the sickest patients you'll ever manage.
- Recall that patients with ESLD have higher rates of infection and worse outcomes.
- Always consider spontaneous bacterial peritonitis (SBP) in the sick patient with ESLD. In fact, SBP is the most common infection in ESLD patients.
- Physician impression alone has been repeatedly shown to be inaccurate in ruling out SBP.
- In the critically ill patient with ESLD and ascites, tap the belly!
Show References
Question
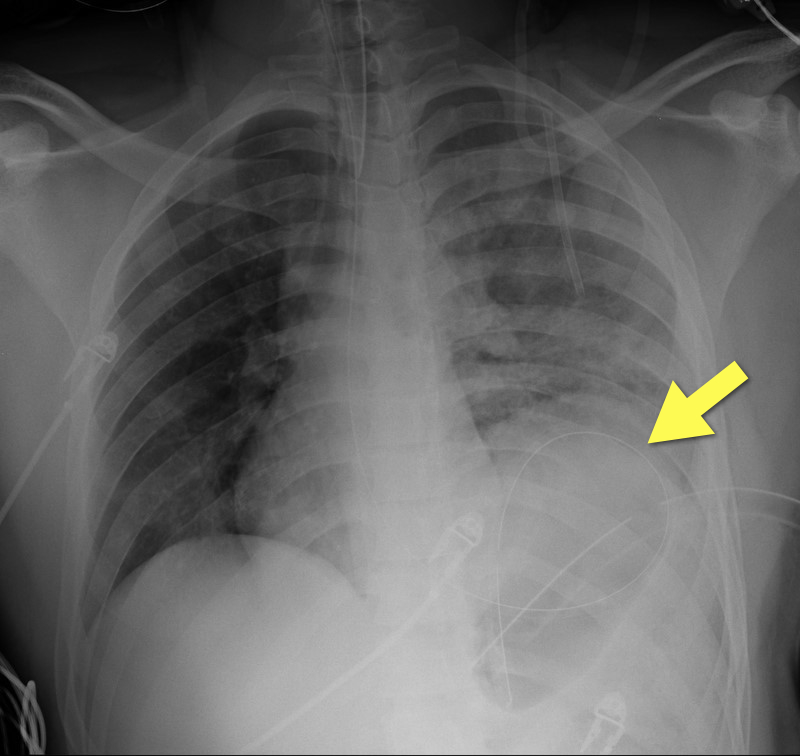
19 year-old male s/p high-speed MVC with hypotension and diminished breath sounds on left. Diagnosis?
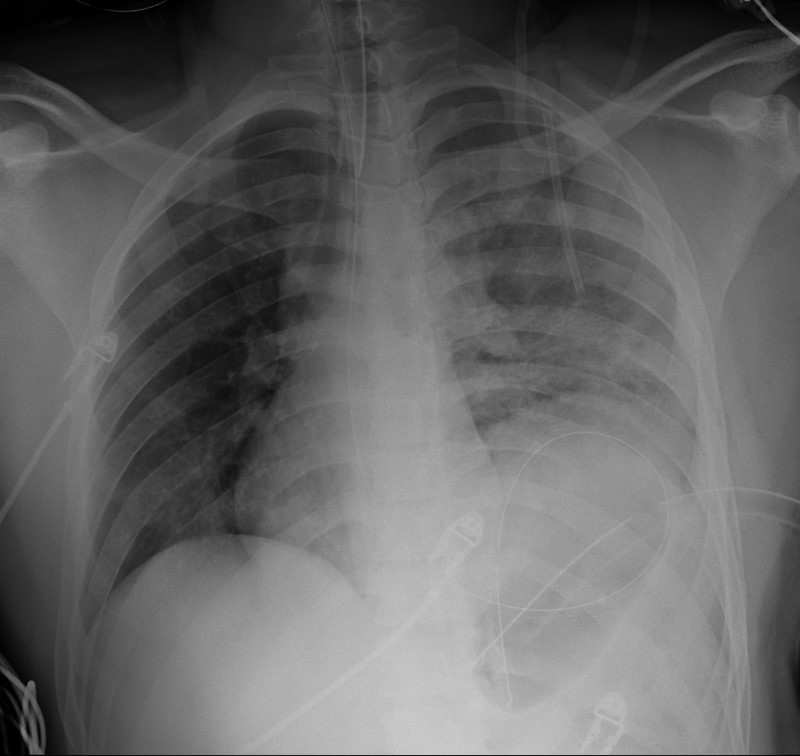
Show Answer
Show References
A patient presents to the ED in pulmonary edema, hypotensive, and has JVD. There's a new systolic murmur. The patient had an acute MI 7-10 days ago and had appropriate treatment and uncomplicated course, then discharge. What's the diagnosis and what do you do?
Step 1: Sign out immediately.
Step 2: If it's not time to sign out (just kidding about step 1), listen carefully to the murmur. If it's heard best at the lower sternal border, it's probably a ruptured papillary muscle with acute MR. If it's a "machinery" type murmur heard throughout the precordium loudly, it's probably an acute VSD.
Step 3: VSD patient is likely to die, but with either one, you've got to move quickly. IMMEDIATELY call cardiology AND cardiac surgery. The patient is in need of a balloon pump and OR.
All you can do is buy time until the patient goes upstairs....pressors for BP, IV NTG as tolerated for preload reduction, and be judicious with diuretics. Vasodilators might help unload the heart also. This patient may end up on 2-3 drips, and make sure ALL meds are titrateable. And just keep your fingers crossed!
Show References
Posterolateral Corner Injuries
The posterolateral corner “PLC” of the knee is becoming increasingly recognized as an extremely important structure to maintain the stability of the knee joint.
PLC injuries occur with hyperextension, varus load and tibial external rotation. So the most common mechanism is a posterolaterally directed blow to the anteromedial tibia when the knee is hyperextended. PLC injuries are commonly associated with injury to other ligaments (ACL, PCL, LCL) and occur in isolation in <5% of cases. If suspected make sure to check for other ligamentous injuries.
Since this injury can be missed and is associated with significant disability it is important to test for it. This YouTube video, http://youtu.be/bnXaTdvZZ6o, demonstrates several examination techniques that can identify the injury.