Search
141-160 of 310 results by Robert Flint
This small study randomized patients with 2 or greater rib fractures or requiring chest tube insertion into a kerorolac (30 mg) or ketamine (0.25 mg/kg) group and evaluated pain levels pre, 30 and 60 minutes post medication administration. They also looked at need for morphine rescue medication. The ketamine group had superior pain control and required less rescue medication.
Show References
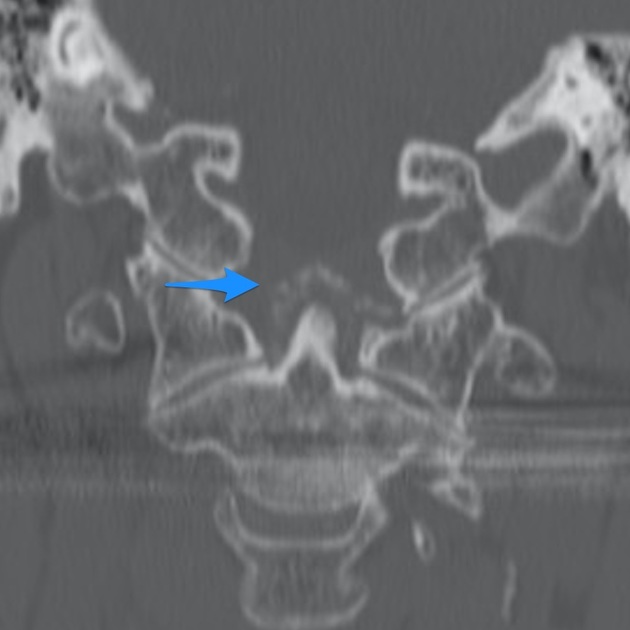
Fractures of the occipital condyles are a relatively rare injury that occur in high energy blunt mechanisms (IE roll over MVC) most commonly. Physical exam will show signs of basilar skull fracture and significant pain at the base of the skull/upper C-spine. CT scan is the gold standard to make the diagnosis. Look for signs of upper extremity weakness on physical exam or cranial nerve injuries. Those type of findings should also prompt emergent MRI evaluation. Treatment generally is long term immobilization in a collar however Type 3 and those with neurologic findings may require surgical intervention.
Anderson and Montesano Classification
Type I 3% of occipital condyle fracturesImpaction-type fracture with comminution of the occipital condyle
Due to compression between the atlantooccipital joint
Stable injury due to minimal fragment displacement into the foramen magnum
Type II 22% of occipital condyle fracturesBasilar skull fracture that extends into one or both occipital condyles
Due to a direct blow to skull and a sheer force to the atlantooccipital joint
Stable injury as the alar ligament and tectorial membrane are usually preserved
Type III 75% of occipital condyle fractures Avulsion fracture of condyle in region of the alar ligament attachment (suspect underlying occipitocervical dissociation)
Due to forced rotation with combined lateral bending
Has the potential to be unstable due to craniocervical disruption

Show References
This meta analysis of studies looking at thrombolytics and prostaglandins in treating significant frost bite offers some insight into the possibilities these therapeutics offer. Unfortunately, the studies available are not high quality and most are case reports.
“Our results suggest that thrombolysis or intravenous iloprost is effective when administered promptly to treat severe frostbite. For grade 3–4 frostbite the Wilderness Medical Society frostbite guidelines recommend the use of intravenous iloprost within 48 h of injury, and thrombolysis within 24 h of injury. The Helsinki protocol recommends the use of tPA for patients with grade 3–4 frostbite presenting within 48 h of injury with angiographic evidence of thrombosis."
“Iloprost is a synthetic prostaglandin I2 that has been used to treat frostbite . Like other prostacyclins, it inhibits platelet aggregation and promotes vasodilation. Iloprost may stimulate the release of endogenous tissue plasminogen activator or counteract its inhibitory effects [35]. Iloprost reduces vasoconstriction induced by thromboxane A2 , and may reduce oxidative stress from free radicals, moderating reperfusion injury [37, 38]. The effect on platelet aggregation may be reversed within two hours), but prostacyclin effects may disrupt the vicious cycle of activated platelets and leukocytes that damages endothelium .”
More research in this area is needed. Transfer to a center with these capabilities seems worth a discussion in the case of severe frostbite.
Show References
The Trauma Frailty Index has been validated to predict inpatient mortality, major complications and discharge to rehab facility. “In addition, frailty was significantly associated with higher adjusted odds of mortality, major complications, readmissions, and fall recurrence at 3 months postdischarge ( p < 0.05).”
It is a simple 15 variable index.

Show References
The level of fitness/health a patient has entering the marathon of recovery from critical illness or trauma has a major impact on morbidity and mortality. Frailty is a measure of this fitness level. The clinical frailty scale can be used to assess your patients ability to survive critical illness. Age is a number. Frailty is more useful.


Show References
This study followed patients presenting to the ED with elevated (SBP>180, DBP>120) blood pressure without evidence of end organ dysfunction for one year. The patients were followed for major adverse cardiac events. They found:
“A total of 12,044 patients were enrolled. The prevalence of MACE within one year was 1,865 (15.5%). Older age, male gender, history of cardiovascular disease, cerebrovascular disease, diabetes, smoking, presentation with chest pain, altered mental status, dyspnea, treatment with intravenous and oral hydralazine, and oral metoprolol were independent predictors for one-year MACE. Additionally, discharge with an SBP ?160 mm Hg was not associated with 30-day MACE-free survival after propensity matching (hazard ratio 0.99, 95% confidence interval 0.78–1.25, P?=?0.92).”
Treating to reach a magic number did not help. Most likely, long term control of blood pressure is a more important factor than attempts to lower in the ED. While this is a high risk group, there is no evidence that acute lowering of blood pressure impacts long term survival.
Show References
This study suggests no. The control arm was given standard physical therapy and the intervention arm was instructed in four basic exercises to do on their own daily for a week. Patents were then surveyed to assess for long term pain. There was no difference in pain between the two groups. Meaning, at least in this study reliant on patient journaling and follow up, that these four simple exercises did not impact long term pain in chest wall injured patients. More work needs to be done in this important area.
Show References
Crowned dens syndrome is an acute inflammatory disease caused by deposition of calcium pyrophosphate dihydrate crystals or hydroxyapatite crystals in the soft tissue and ligaments surrounding the dense. Patient presentation is severe pain in the neck and base of the skull, low grade fever, and elevated inflammatory markers. It is most commonly seen in elderly females. Ct scan is the gold standard for diagnosis. Once meningitis and other significant infectious process has been excluded, treatment is anti inflammatory medications including steroids.
Show References
Another large database evaluation of the use of etomidate vs. ketamine as an induction agent for intubation found a trend toward higher mortality in the etomidate group. Even when trying to control for steroid use (to control for etomidate’s possible adrenal suppression), etomidate had a higher mortality rate.
A well done study that adds to the chorus advocating for choosing ketamine when looking for a hemodynamically neutral induction agent.
Show References
In this randomized trial of restrictive oxygen (arterial oxygen sat of 94% ) vs. liberal oxygen (12-15 L of O2 per minute) for 8 hours after traumatic injury there was no difference in mortality or major respiratory complications at 30 days between the two groups.
Further evidence that managing hypoxia is important but over oxygenation at best offers no benefit and may add harm.
Show References

This prospective observational study looked at patients with liver lacerations and active contrast extravasation who either had immediate embolization vs. observation. After matching for age, injury score etc. the observation first approach did as well as those who had immediate embolization.
Show References
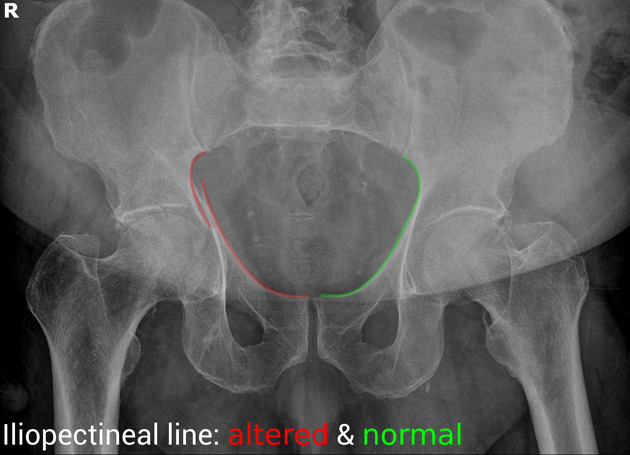
This study tried to expand upon what they describe as the classic triad of signs to diagnose ruptured AAA “(1) abdominal pain, (2) hypotension and (3) a pulsatile abdominal mass”. They tested these against the _modified abdominal aortic aneurysm rupture signs. “_The MARS-signs encompassed (1) the registered pain-associated symptoms or signs, (2) all hypovolemic associated signs, and (3) pulsatile abdominal mass and/or ultrasound finding”. The MARS did slightly better in identifying ruptured AAA retrospectively. For me, this doesn’t add a great deal of help in making this can’t miss diagnosis and further work is necessary.
Show References
Question
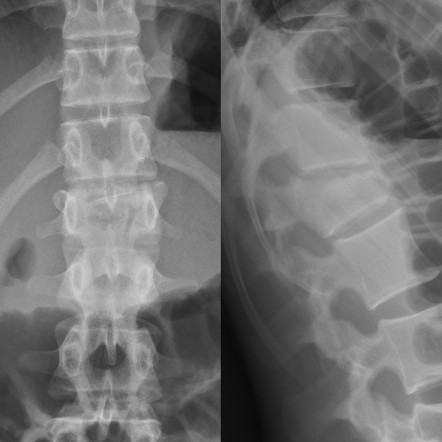
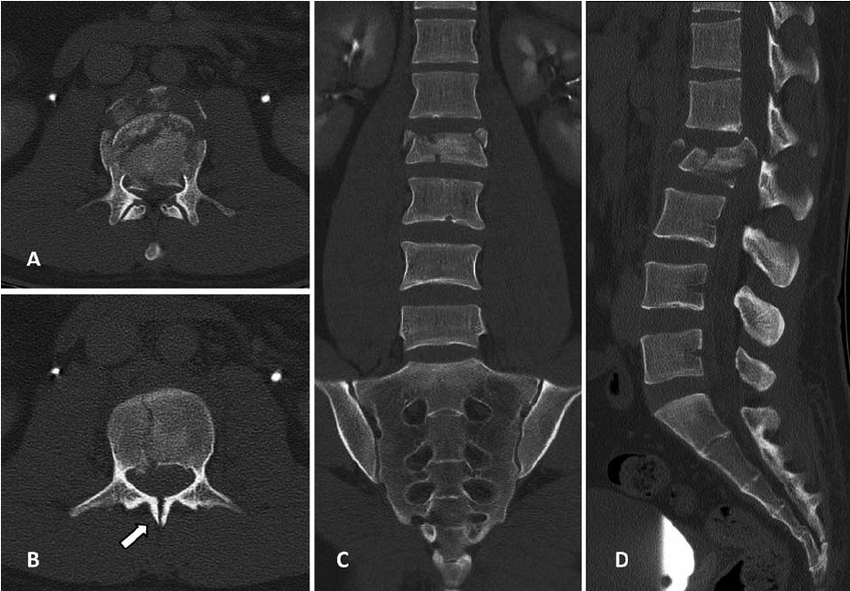
Fall from a height of 6 feet with back pain. Plain film shown. What is the diagnosis? Any further imaging indicated? Treatment? Disposition?
Show Answer
Show References
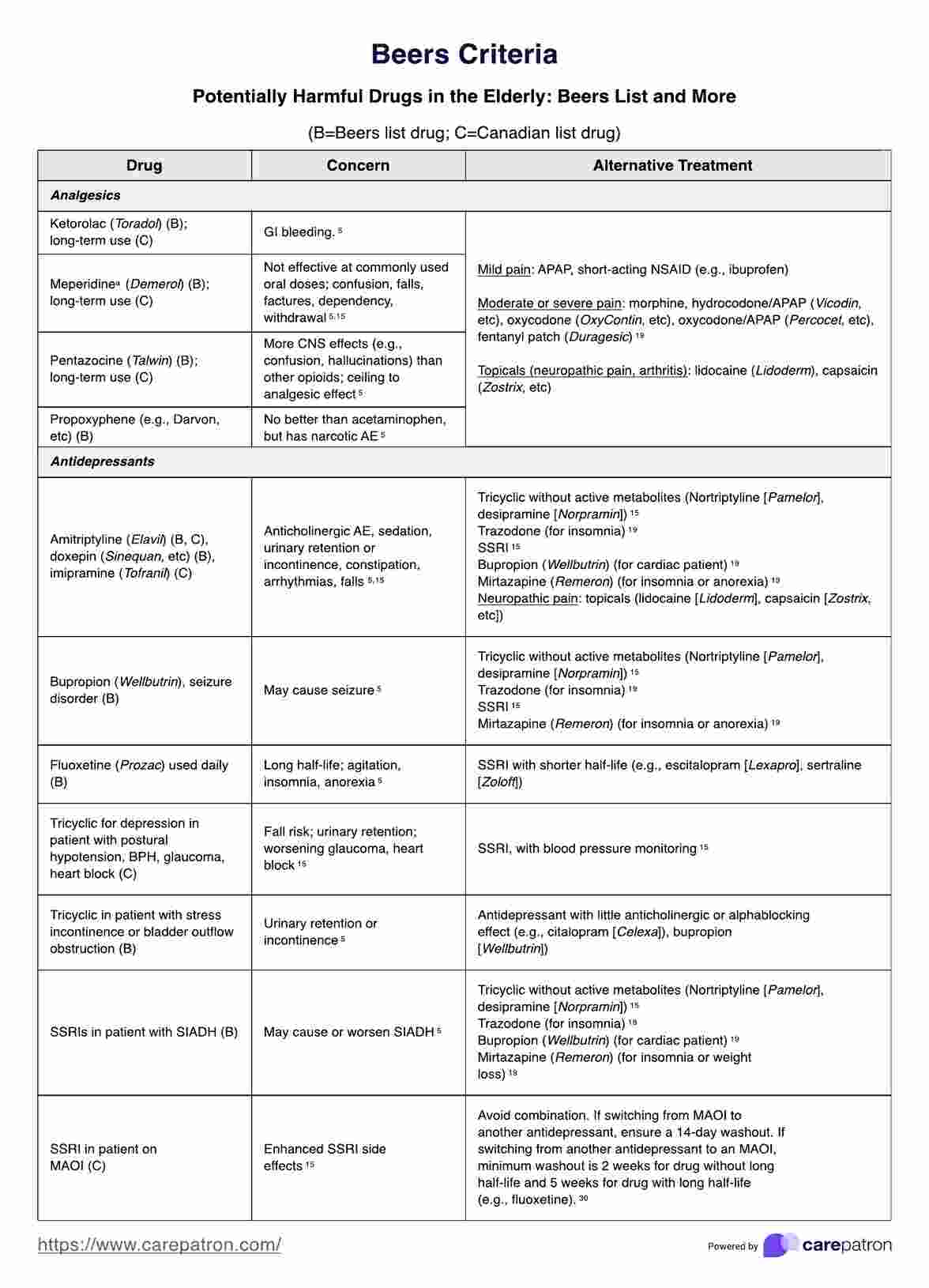
As a reminder, prescribing medications to older patients should be done with caution because of changed physiology, co-morbid conditions and other currently used medications. The Beers Criteria is a helpful list of medications that may cause trouble for your older patients. https://www.guidelinecentral.com/guideline/340784/#section-2776198 is a list of medications to either avoid or prescribe carefully in this patient population.
Pay particular attention to medications that have anticholinergic properties as they cause change in mental status and increase the risk for falls.
Show Additional Information
{kind=link}
Show References
From all of us at UMEM, Happy Thanksgiving!!
We are incredibly Thankful for each of you and all that you do to care for patients and their families.
We are Thankful for those legends who have blazed the path in EM like Greg Henry who the EM community lost yesterday. Our thoughts are with his family. Thank you Dr. Henry for inspiring so many of us. Our pearls today are two of his famous quotes:
“Medicine is show business for ugly people.”
“You don’t go to Disney and see Mickey taking a smoke break. You have to be on when you are on shift”
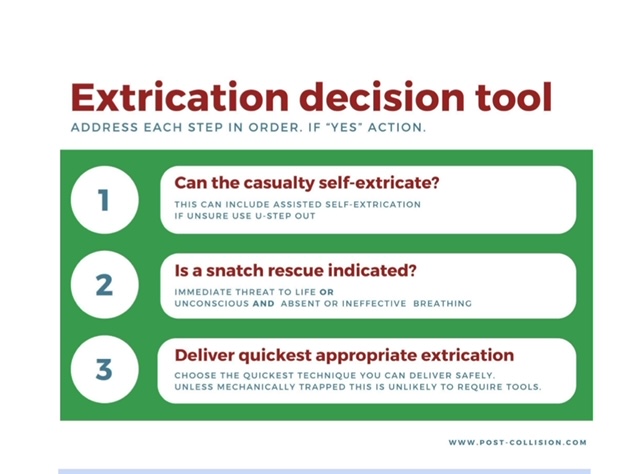
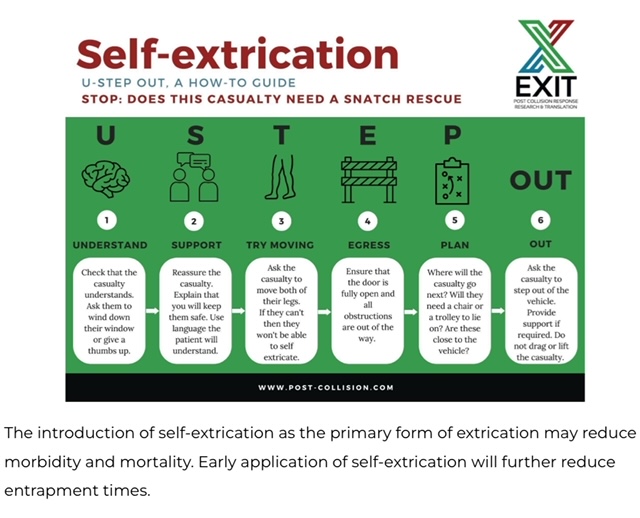
It is important for trauma and emergency care providers to understand what our patients experience prior to arrival in our clean, safe, and structured emergency department. It is also vitally important that we are involved in training and education in the pre-hospital environment. A group in the United Kingdom is challenging the age old “wisdom” that post-motor vehicle crash extrication should be slow, methodical, and work to have absolutely no movement in the spinal canal. Spinal immobilization and slow extrication instead of rapid resuscitation appears to be bad for patients. Based on several of their ground breaking papers they have published a 14 point recommendation of patient extrication post motor vehicle collision. Here are two important tenets they propose. For an in-depth discussion check out November 14, 2024 / CPD, Podcasts, Roadside to Resus.
Show References
The authors looked at 51 patients intubated with both anterior and posterior cervical collar in place and measured the degree of movement within the spine during intubation. They repeated this process in 51 additional patients with just the posterior portion of the collar in place. They found there was one degree of difference in movement between the two groups. This adds evidence that removing the anterior portion of the collar is safe when intubating trauma patients.
Show References
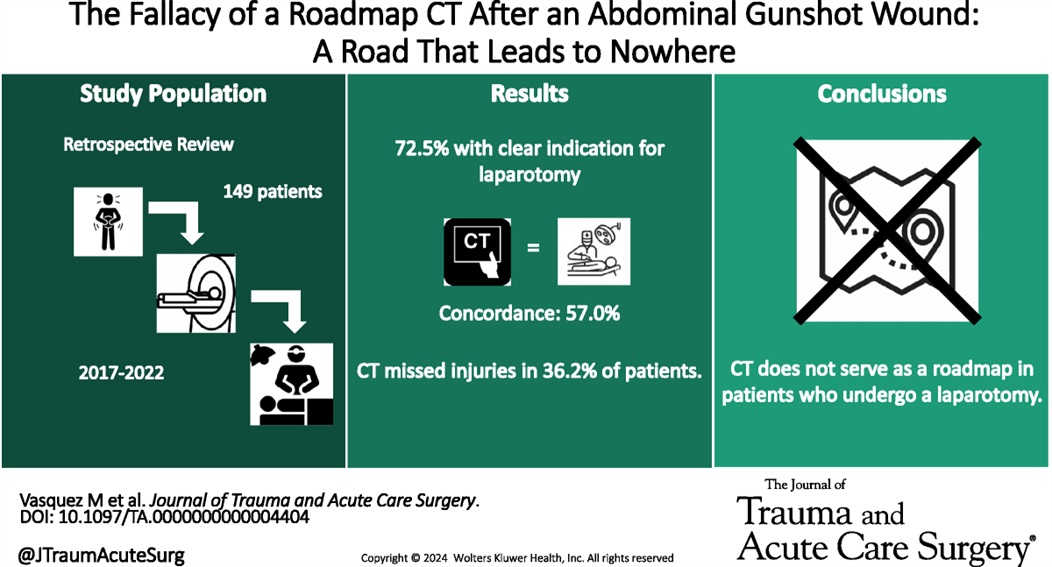
This retrospective study illustrates that the use of CT scanning to identify injury in gun shot wounds to the abdomen is not sensitive or specific enough to obviate the need for laparotomy. “Admission hypotension, abdominal pain and/or peritonitis, evisceration, and a transabdominal trajectory were considered clear indications for laparotomy.” If there is clear indication to go to the OR, stopping in CT does not add any benefit.
Show References
Administration of prehospital TXA was found to improve 28 day mortality and decrease the amount of blood required to be transfused without any increased risk of thromboembolism or seizure. Two grams of TXA was superior to one gram and no TXA.