Search
The American College of Medical Toxicology's ToxIC Registry is a self-reporting database completed by medical toxicologists across 69 insitutions in the US.
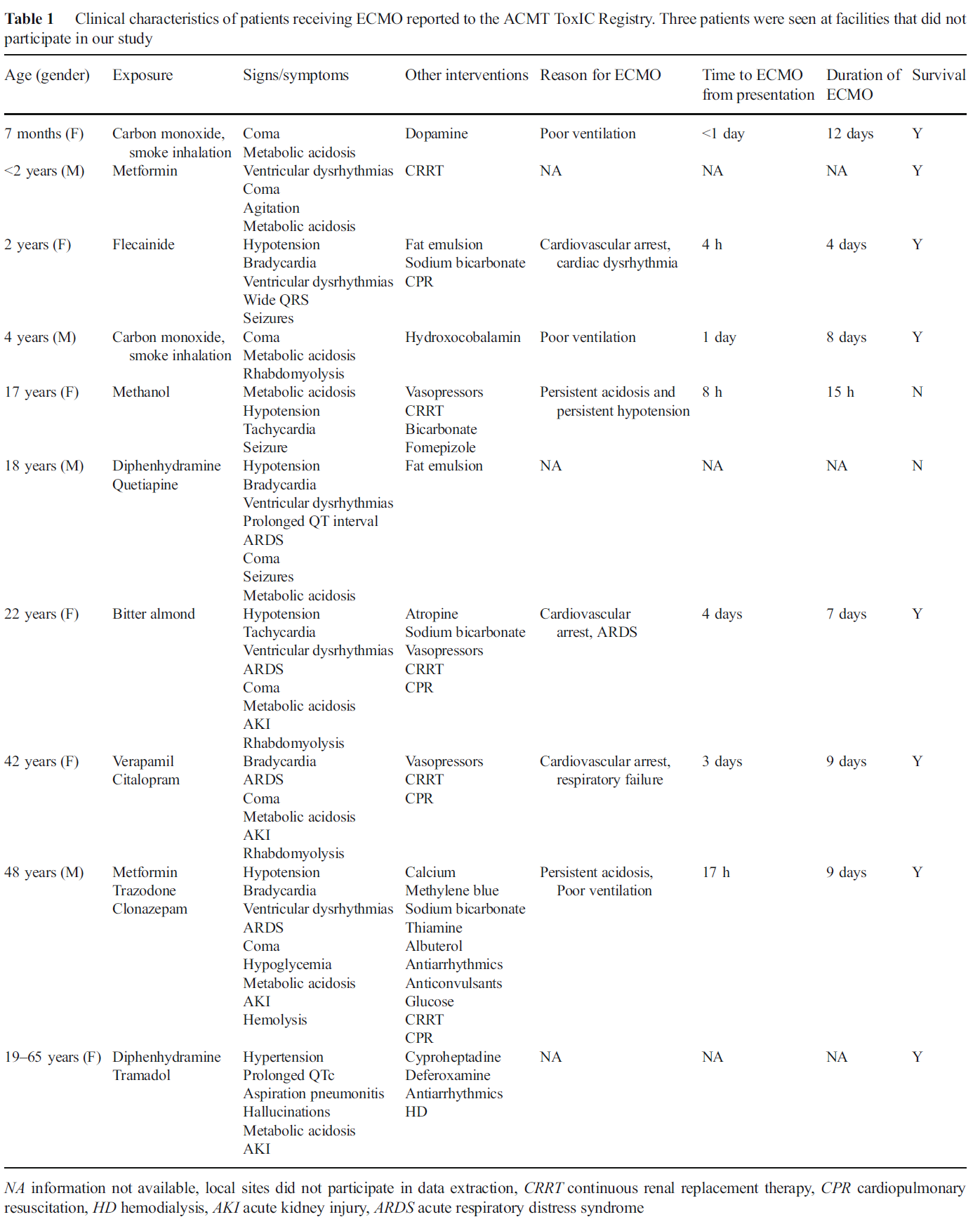
- Over a 3 year period, just 10 cases in the database received ECMO: 4 pediatric, 2 adolescent, and 4 adults (individual cases presented in the table below)
- Time of initiation of ECMO ranged from 4 h to 4 days, with duration from 15 h to 12 days
- Exposures included carbon monoxide/smoke inhalation (2), bitter almonds, methanol, and several medications including antihistamines (2), antipsychotic/antidepressant (2), cardiovascular drugs (2), analgesics (2), sedative/hypnotics (2), and antidiabetics (2)
- Overall survival rate was 80%
Application to Clinical Practice
In settings where ECMO is available, it may be a potential treatment option in severely poisoned patients. From the limited data, ECMO was generally administered prior to cardiovascular failure and might be of benefit particularly during the time the drug is being metabolized.
Table from the Case Series
Show References
What Do You Mean By Dizzy?
- Patients with dizziness account for 3% of ED visits.
- The traditional approach based on symptom quality (i.e. “What do you mean by dizzy”) is not reliable.
- Drs. Edlow and Newman-Toker propose a new paradigm based on the timing and triggers of dizziness.
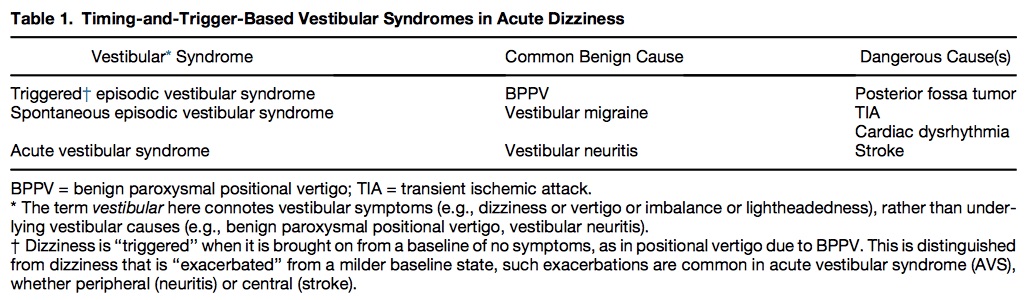
- Acute vestibular syndrome begins abruptly or rapidly and continues for days. Patients’ dizziness may be exacerbated by movement but is not triggered by movement.
- Triggered episodic vestibular syndrome are repetitive episodes of dizziness triggered by some event. Patients will be completed asymptomatic at rest and will develop dizziness that is reliably triggered by a specific event or postural shift.
- Spontaneous episodic vestibular syndrome are multiple episodes of dizziness that occur without any clear identifiable trigger. Patients are asymptomatic between episodes.
Table 1 shows common benign and serious causes of these vestibular syndromes.
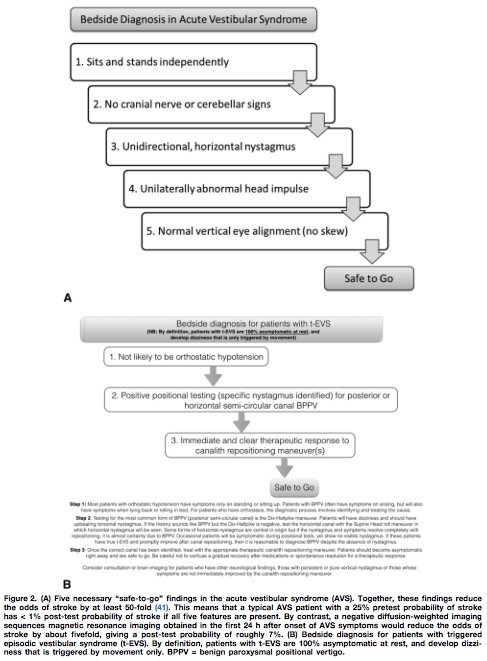
Utilizing the HINTS battery or the Dix-Hallpike maneuver, a “safe to go” algorithm for acute vestibular syndrome and triggered episodic vestibular syndrome is outlined in Figure 2.
Show References
Attachments
Disclaimer: Talking about seizures/status that is NOT due to eclampsia
- Propofol (Class B) -- though not recommended for obstetric use by manufacturer
- Benzodiazepines (Class D) -- mostly due to fetal withdrawal syndrome, but some teratogenicity to prolonged exposure inconsistent in literature
- Ketamine (No FDA class assigned but likely Class B Austrailia equivalent)
- Levetiracetam (Class C) -- no clear evidence of major fetal malformations in humans
- Phenytoin, phenobarbitol, carbemazepine, valproic acid and most other common AEDs (Class D due to teratogenicity)
TAKE HOME: While no AEDs are completely safe in pregnancy, treatment and stabilization of maternal status epilepticus is paramount for fetal health. Involve neurology/epileptology and OB/maternal-fetal medicine.
Show References
Orthopedic documentation
1) Document location with specificity and laterality.
2) Document the location with as much specificity as possible
-Name of specific bone and specific site on bone (Shaft, head, neck, distal, proximal, styloid)
3) Document fractures as open/closed, displaced vs. non-displaced, routine or delayed healing,
-Orientation of fractures, such as transverse, oblique, spiral
- Document intra-articular or extra-articular involvement
4) For a particular injury, a complete note will include mention of the following
The joint above (e.g. for shoulder injuries this would be the neck, for hip injuries - the back)
The joint below
Motor (e.g. for arm injuries document the distal median, radial and ulnar motor innervation)
Sensory
Vascular
Skin (for all fractures document intact overlying skin esp. when covering with a splint)
Compartments (a simple mention of compartments are grossly soft/not tense will suffice)
*Especially relevant for forearm and tib/fib injuries
[CORRECTION]: Versed dose is 2-2.5 mg total not mg/kg
Patients with severe agitation present a unique challenge to the emergency department. Acute delirium is often due to psychostimulants such as cocaine, amphetamines, PCP, or synthetic cannabinoids, alcohol, or psychiatric illness. These patients require urgent evaluation necesssitating the use of physical and chemical restraints, not only for their own safety but also the hospital staff's. Fingerstick glucose, pulse oximetry, and vital signs must be expeditiously obtained. Severely agitated combative patients who are physically restrained are at high risk for morbidity from asphyxiation, hypermetabolic consequences (acidosis, hyperthermia, rhabdomyolysis), and death can occur.
Ketamine is phencyclidine derivative that causes dissociative state between the cortical and limbic systems which prevents the higher centers from preceiving visual, auditory, or painful stimuli. Ketamine has a wide safety profile and has been used worldwide for many years with few complications. It possesses ideal characteristics for rapid sedation of agitated patients:
- Rapid onset of action 1-3 minutes
- Preservation of airway reflexes
- Lack of respiratory or cardiac depression or QT prolongation
- Short half-life of 30-40 minutes
- Safe in situations with minimal to no monitoring
- Dose: Intravenous =1.5-2 mg/kg Intramuscular = 5-6 mg/kg (maximum 400 mg)
Experience with Ketamine in patients with excited delirium has shown good initial control of agitation however, patients often require additional medications for deeper or longer duration of sedation. Benzodiazepines are recommmended as second line agents particularly intravenous or intramuscular Midazolam 2-2.5 mg /kg.
Show References
As noted previously, injuries cause substantial morbidity and mortality globally. How does it vary by age group?
The following table shows that unintentional injuries are the leading cause of death for individuals 1-44 years of age. Even when they are not the leading cause of death, injuries cause substantial mortality in all age groups.
Show References
- Amiodarone and lidocaine are commonly used antiarrhythmics for ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). Their efficacy towards survival to hospital discharge and neurological outcome, however, has been questioned.
- A recently published study in the NEJM evaluated these drugs by performing a double-blind, randomized, placebo-control trial. The trial evaluated patients presenting with out of hospital cardiac arrest secondary to VF or pulseless VT that is refractory to one or more shock.
- The trial randomized 3,026 patients to receive amiodarone (974), lidocaine (993), or normal saline (i.e., placebo) (1,059); the primary outcome was survival to hospital discharge and the secondary outcome was favorable neurological outcome at hospital discharge. Several sub-group analyses were planned a priori.
- No statistically significant difference was found in hospital survival or neurologic outcomes between any of the groups. Patients who had a witnessed arrest and bystander CPR had higher rates of survival with either lidocaine or amiodarone compared to saline while there was no difference between the two.
Show References
Guidelines recommend loading doses of vancomycin (15-20 mg/kg, up to 30 mg/kg in critically ill patients), but the risk of nephrotoxicity is unknown. A new retrospective cohort study aimed to compare nephrotoxicity in ED sepsis patients who received vancomycin at high doses (>20 mg/kg) versus lower doses (20 mg/kg).
What They Found
-
1,330 patients had three SCr values assessed for the primary outcome
-
High-dose initial vancomycin was actually associated with a lower rate of nephrotoxicity (5.8% vs 11.1%)
-
After adjusting for age, gender, and initial SCr, the risk of high dose vancomycin compared to low dose was decreased for the development of nephrotoxicity (RR=0.60; 95% CI: 0.44, 0.82)
Application to Clinical Practice
It appears initial loading doses of vancomcyin > 20 mg/kg do not cause increased risk of nephrotoxicity.
Show References
Emergency medicine remains a relatively young and developing specialty in most parts of the world. However, it is growing in popularity, especially in the U.S. How competitive is it currently?
For the recent 2016 Match, there were 2476 applicants for 1895 categorical emergency medicine positions from 174 programs.
- Of the 1895 incoming residency positions, 1894 were filled within the Match!
- The vast majority (78.4%) were filled by senior medical students coming directly from U.S. medical schools.
Bottom Line: Emergency medicine remains a highly desired and competitive specialty in the U.S.
Congratulations to all the incoming interns for the 2016-2017 year!
What is cardio-renal syndrome CRS?
- Covers disorders where acute or long-term dysfunction of one organ can cause acute or long-term dysfunction of the other
- Worsening renal failure, diuretic resistance in heart failure, and worsening kidney function during heart failure are all characteristic of the disease process
There are 5 types
1. Acute CRS: abrupt worsening of heart function leading to kidney injury
2. Chronic CRS: chronic heart failure leads to progressive kidney disease
3. Acute renocardiac syndrome: abrupt kidney dysfunction leading to acute cardiac disorder
4. Chronic renocardiac syndrome: chronic kidney disease leading to decreased cardiac function
5. Systemic CRS: Systemic condition leading to both heart and kidney disease
Show References
Metacarpal Fractures
* Localize fracture to head, neck or shaft (neck most common)
5th metacarpal most commonly fractured
* Note amount of angulation, shortening and the presence of malrotation
*Treatment is based on which metacarpal is fractured and the location of the fracture
*The amount of acceptable angulation varies by the digit involved
For example for index and long finger - acceptable angulation of the shaft is 10-20 degrees and neck is 10 to 15 degrees
Whereas for the 5th digit - acceptable angulation for the shaft is 40 degrees and neck is 50 degrees
Pearls
No degree of malrotation is acceptable (document the absence of this!)
Strongly suspect fight bite injury with abrasions/lacerations overlying metacarpal heads
Highly prone to infection given the proximity to the joint capsule
Consider lacerations over metacarpal fractures as open fractures (do not close/discuss management with hand surgery re timing of washout. Many prefer delayed fixation for suspected infections )
Document integrity of the extensor tendon (can be lacerated and retracted)
Show References
Cerebral Venous Thrombosis
- Approximately 25% of patients with cerebral venous thrombosis (CVT) will experience neurologic deterioration.
- This is most commonly due to an increase in ICP that results in transtentorial herniation.
- While heparin remains the treatment of choice for CVT, consider the following alternative strategies in the acutely decompensating patient:
- Endovascular thrombolysis
- Mechanical thrombectomy
- Decompressive hemicraniectomy
Show References
A meta-analysis of 74 randomized trials with a total of 58,556 patients was recently published in the Lancet that looked at the effectiveness of NSAIDs in the treatment of osteoarthritis (OA) pain.
Briefly, their conclusion was that:
- Acetaminophen is ineffective as a single-agent in the treatment of OA.
- Diclofenac 150 mg/day had best evidence to support it as the most effective NSAID available presently with respective to its effectiveness in relieving pain and improving function.
- They found no evidence that treatment effects varied over the duration of treatment ( no tolerance)
You can find the article here http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2816%2930002-2/abstract
Show References
A previous pearl has looked at serum HCO3 as a predictor of DKA (see pearl from 8/21/15). The article by Gilhotra looks at using end tidal CO2 (ETCO2) to exclude DKA. 58 pediatric patients were enrolled with 15 being in DKA. No patient with ETCO2 > 30 mmHg had DKA. Six patients with ETCO2 < 30 mmHg did not have DKA. Other studies done in children have shown similar results.
An article recently published by Chebl and colleagues examined patients older than 17 years with hyperglycemia. In this study, 71 patients were included with 32 having DKA. A ETCO2 >35 excluded DKA in this group while a level <22 was 100% specific for DKA.
Bottom line: ETCO2 >35 mmHg is a quick bedside test that can aid in the evaluation of hyperglycemic patients.
Show References
Cutaneous larva migrans (CLM) is an acquired dermatosis
- Seen in patients returning from the tropics
- Often seen in patient with a history of sunbathing or in barefoot beachgoers
- Caused by the larvae of various nematode parasites of the hookworm family (Ancylostomatidae), with Ancylostoma braziliense the most frequently found in humans.
Clinical manifestations:
- Linear, serpentine erythematous lesions
- Intense pruritus
- Will often heal spontaneously over weeks or months without treatment
Treatment:
- Thiabendazole (applied topically)
- Oral alternatives include other anti-parasitic medications such as albendazole, ivermectin
- Oral thiabendazole as a single dose can be used, but is less effective than albendazole or ivermectin
- Consider antibiotics if there is secondary bacterial infections
- Freezing the leading edge has been previously used, but is considered ineffective and painful.
Bottom Line:
- Consider CLM the next time a patient complains of a linear, erythematous itchy rash after returning from their all-inclusive stay in a Caribbean resort
Show References
Attachments
There are multiple vasoactive infusions available for acute hypertensive emergencies, many having serious side effect profiles or therapeutic disadvantages.
Clevidipine (Cleviprex) is rapidly-titratable, lipid-soluable dihydropyridine calcium channel blocker which has become increasingly used in the ICU in recent years [1]:
- Onset of action 2-4 minutes
- Duration of action 5-15 minutes (half-life of 1 minute)
- Clevidipine is relatively inexpensive ($108/50mL bottle)
- Side effects include hypertriglyceridemia, hypotension and reflex tachycardia
ECLIPSE trial compares clevidipine, nicardipine, nitroglycerin and nitroprusside in cardiac surgery patients. .
Clevidipine was as effective as nicardipine at maintaining a pre-specified BP range, but superior when that BP range was narrowed (also studied in ESCAPE-1 and ESCAPE2 with similar results) [2-3]
TAKE-HOME: Clevidipine is an ultra short-acting, rapidly-titratable vasoactive with favorable cost, pharmacokinetics, and side-effect profile. Consider its use in hypertensive emergencies.
Show References
Femoral neck fracture
- The most commonly missed hip fracture
We typically think of the presentation of the displaced fracture severe pain, writhing in the bed, unable to ambulate, limited ROM
* However, patients with nondisplaced fractures (15 20%) may walk with a limp
* Occurs primarily in the elderly & osteoporotic population after a fall directly onto the hip
* Look for a cortical step-off in the femoral neck (w/ foreshortening)
* A patient with a minimally displaced fracture may only complain of hip, knee, or groin pain and may be able to walk (albeit with a limp)
* Almost 9% of hip fractures are radiographically normal (Nondisplaced or impacted fractures)
* Fractures which were initially nondisplaced, may become displaced upon re-presentation
* Remember the limitations of plain x-ray in the evaluation of femoral neck fractures!
* Because of the significant complication of overlooking a femoral neck fracture, MRI has become the recommended imaging modality of choice for a patient with a high suspicion for a femoral neck fracture, despite normal plain radiographs of the hip
Acute cocaine toxicity can manifest with several cardiovascular issues such as tachycardia, dysrhythmia, hypertension, and coronary vasospasm. A new systematic review collated all of the available evidence for potential treatment options. Here is what the review found (there is also an 'other agents' section for medications with less published reports):
-
Benzodiazepines and other GABA-active agents: Benzodiazepines may not always effectively mitigate tachycardia, hypertension, and vasospasm from cocaine toxicity.
-
Calcium channel blockers: Calcium channel blockers may decrease hypertension and coronary vasospasm, but not necessarily tachycardia.
-
Nitric oxide-mediated vasodilators: Nitroglycerin may lead to severe hypotension and reflex tachycardia.
-
Alpha-adrenoceptor blocking drugs: Alpha-1 blockers may improve hypertension and vasospasm, but not tachycardia, although evidence is limited.
-
Alpha-2-adrenoceptor agonists: There were two high-quality studies and one case report detailing the successful use of dexmedetomidine.
-
Beta-blockers and alpha/beta-blockers: No adverse events were reported for use of combined alpha/beta-blockers such as labetalol and carvedilol, which were effective in attenuating both hypertension and tachycardia.
-
Antipsychotics: Antipsychotics may improve agitation and psychosis, but with inconsistent reduction in tachycardia and hypertension and risk of extrapyramidal adverse effects.
-
Sodium bicarbonate: Twelve case reports documented treatment of dysrhythmia with IV sodium bicarbonate, with seven reporting successful termination.
The authors note that "publication bias is a concern, and it is possible that successful treatment and/or adverse events have not been reported in some of the publications, and in general."
Show References
Sunset Eye Sign
- The "sunset eye sign" can be seen in patients with increased intracranial pressure related to obstructive hydrocephalus or shunt malfunction.
- It describes an up-gaze paresis caused by compression of the dorsal midbrain.
- The lower portion of the pupil may be covered by the lower eyelid, appearing like a setting sun.