Search
The Importance of Antibiotic Timing for Sepsis and Septic Shock
- Septic shock is perhaps the most common critical illness that emergency physicians manage.
- In several studies, delays in initiating antibiotics for patients with septic shock were the strongest predictor of mortality.
- Broad spectrum antibiotics should be administered ASAP (preferably within 60 minutes) to patients with septic shock.
- Selection of antibiotics should be based on the presumed source, the antibiogram at your institution, and the patient's risk factors for resistant organisms.
Show References
Diagnosing Subarachnoid Hemorrhage-6 Pitfalls
1. Subarachnoid hemorrhage (SAH) doesn't always present as the "worst ever" headache. Don't most of our patients say their headache is the worst headache anyway? Be suspicious of the diagnosis if your patient has acute onset of an unusual or atypical headache. Diagnoses starts with the history.
2. The neuro exam may be completely normal in some cases, especially early on.
3. The headache due to SAH may get better with analgesics. This is a huge pitfall. Don't rule this diagnosis out if analgesics help.
4. The CT scan may be negative. Enough said.
5. Be careful with interpretation of the CSF. We all want the number of red cells in tube 4 to be zero. Be careful with this. Although the rbcs may have dropped by 50% from tubes 1 to 4, the diagnosis hasn't been excluded unless the cells clear completely. Although there have been some case reports of SAH with rbcs < 100, this is pretty uncommon.
6. CT Angiography and/or MRI with FLAIR is not a substitute for the lumbar puncture.
Show References
![]()
Dear Readers,
Thank you for your continued interest in the University of Maryland's EM Pearls program. We are conducting a survey to assess whether our pearls are meeting your needs. Data collected will be used to refine and improve our educational program. Please take 1 minute to complete our survey by clicking the link below.
http://umem.org/surveyor/index.php?sid=86815&newtest=Y&lang=en
If you regularly forward pearls to other readers, please forward this message as well. We wish to capture as many readers' opinions as possible.
If you have any questions or problems, please contact: admin@umem.org
Sincerely,
Dan Lemkin, MD MS
EM Pearls Development Team
University of Maryland School of Medicine
Department of Emergency Medicine
Cervical Radiculopathy
The most commonly affected level is C7 (31-81%), followed by C6 (19-25%), C8 (4-12%) and C5 (2-14%)
Anterior compression can selectively affect motor fibers
Posterior compression can selectively affect sensory fibers
-More common due to posterior lateral disc herniation or facet degeneration
Signs and symptoms: Sensory complaints (findings are in a root distribution) and possible weakness and reflex changes.
Show References
In the past several years it has become common practice to use cuffed tubes for pediatric intubations. However, a recent study suggests that cuff pressures are not as well regulated in pediatric patients, particularly when the patients are quickly intubated prior to aeromedical transport. Cuff pressures >30 cm H2O are associated with tracheal damage, however, up to 41% of pediatric patients transferred had cuff pressures >30 cm H2O, and 30% of those had pressures >60 cm H2O!
So:
-
Check your cuff pressures in all patients, particularly prior to transport
-
Cuff pressures must be <30cm H2O
-
Recall that for years uncuffed tubes were the standard, so as long as effective ventilation is achieved, it is best to err on the low side...
If you work at a facility that routinely transfers out the sickest pediatric patients, you will save their life by securing an airway in this most stressful of circumstances, but careful attention to this seemingly small detail can save your patient from long term complications.
Show References
Most cases of normal anion gap metabolic acidosis result from either urinary (RTA) or gastrointestinal HCO3- losses (diarrhea). A number of xenobiotics can also cause this disorder:
- Acetazolamide
- Acidifying Agents: Ammonium chloride, arginine hydrochloride, hydrochloric acid, lysine hydrochloride
- Cholestyramine
- Toluene
- Topiramate (Topamax)
- Transverse Myelitis (TM) is the development of grey and white matter inflammation of the spinal cord, which can result in demyelination.
- Hallmark characteristics of this condition include: (1) isolated spinal cord (not brain) dysfunction, and (2) the lack of associated cord compression.
- TM can be acute or subacute, such that it progresses over the course of hours to several days. Nearly half of cases will reach its maximal deficit within 1 to 10 days of onset.
- The diagnosis of TM is primarily based on the history and physical examination findings. MRI of the spinal cord and myelography are often used as diagnostic adjuncts.
- This condition typically presents with paresthesias, back pain, and ascending leg weakness.
- Febrile illnesses often serve as a precursor; one series found this to be the case in 37% of complete TM cases.
- While steroids are sometimes administered over the first several days of illness to decrease inflammation, there is no cure for TM and treatment is largely supportive in nature.
Show References
Linezolid is used for gram-positive infections resistant to conventional therapy (e.g., Vancomycin-resistant enterococcus and Methicillin Resistant Staph Aureus). Linezolid is an oxazolidinone, but more importantly it is a weak monoamine oxidase inhibitor (MAOI) and serotonin syndrome (e.g., altered mental status, neuromuscular abnormalities, autonomic instability) may occur when combined with selective serotonin re-uptake inhibitors (SSRIs) or with recent discontinuation of SSRI.
Be aware that the following drugs can precipitate serotonin syndrome when combined with Linezolid:
Mirtazpine Buproprion Fentanyl
Trazodone Buspirone Bromocryptine
Levodopa Lithium Amphetamines
Cocaine Codeine Reserpine
Ergots MAOI's
Show References
Got Symptomatic Hypertension? Why not try Fenoldopam?
Fenoldopam is a rapid-acting vasodilator.
- It is an agonist for D1-like dopamine receptors and binds with moderate affinity to α2-adrenoceptors.
- Effective as nitroprusside, however, it has the advantages of increasing renal blood flow (6 times as potent as dopamine in producing renal vasodilitation) and sodium excretion
- Not associated with the accumulation of toxic metabolites, and not requiring shielding from light.
- Fenoldopam can be safely used in all hypertensive emergencies, and may be particularly beneficial in patients with renal insufficiency.
Dosing (Adult): After a starting dose of 0.1 to 0.3 mcg/kg/minute, the dose is titrated at 15 minute intervals, depending on the BP response. May be increased in increments of 0.05 to 0.1 mcg/kg/minute every 15 minutes until target blood pressure is reached. Maximal infusion rate reported in clinical studies: 1.6 mcg/kg/minute.
Onset/duration: 5-10 minutes/~ 1 hour.
Show References
In order to minimize interruptions in compressions due to pulse checks, continuous end tidal CO2 (ETCO2) monitoring during compressions is recommended. Before spontaneous circulation returns, the ETCO2 is likely to be on the order of < 10 mmg Hg. At the moment spontaneous circulation returns, the ETCO2 is expected to abruptly increase to at least 35-40 mm Hg. Be wary, though, that the administration of sodium bicarbonate may transiently increase the ETCO2 even in the absence of return of spontaneous circulation (ROSC).
Use of ETCO2 in this manner allows one to assess the patient for ROSC without ever having to stop compressions for pulse checks.
Show References
Dr. Corwell covered Spondyloysis in July 2010 https://umem.org/res_pearls_referenced.php?p=1134 but if you are like me you might have trouble remembering the differences between the following terms:
- Spondyloysis: A unilateral or bilateral defect in the pars interarticularis portion of a vertebrae. Typically L5 or L4.
- Spondylosis: is a term referring to degenerative osteoarthritis of the joints between the spinal vertebrae and/or neural foraminae.
- Spondylolisthesis: describes the anterior displacement of a vertebra or the vertebral column in relation to the vertebrae below. Usually due to spondyloysis or a fracture of the pedicles of the vertebrae. Can occur anywhere along the vertebral column. Most common at the L4 and L5 level. For example, a hangman's fracture is a spondylolisthesis of the C1 vertebra being displaced anteriorly relative to the C2 vertebra.
- Spondylitis: is an inflammation of the vertebra. As can be seen with ankylosing spondylitis, Pott’s disease or any infection or arthritic disorder of the spine.
Show References
We've all been there. It's 2am, and a 4 week old with a temperature of 38.1 rolls in the door. You grab the LP kit and your "best holder." This person then holds the baby's head and neck flexed with one hand, while the other brings the bottom and legs up to the chest as much as possible...all, usually, without pulse oximetry monitoring.
- By ultrasound, the largest interspinous space is achieved in the upright, hips flexed position (ie. leaning forward).
- In the lateral decubitus position (often preferred in young infants), neck flexion DOES NOT increase the interspinous space.
- Furthermore, neck flexion increases the incidence of respiratory compromise and hypoxia.
Show References
Toxic Holiday Plants
Of the three plants listed, which is NOT poisonous?
1. Holly plant
2. Poinsettia
3. Mistletoe
Poinsettia plants were once thought to be very poisonous. Contrary to popular belief, poinsettias are safe to have in the home during the holidays.
Although there are reported cases of death with ingestion of Holly plants in older literature, recent experience shows gastrointestinal effects in small doses, and serious toxicity such as CNS depression in large ingestions.
Mistletoe ingestion of few of the berries would, at most, produce mild gastroenteritis; however, ingesting concentrated extracts of the plant, including the berries, may produce serious effects such as seizures, mental confusion, drowsiness, and hallucinations.
Happy holidays!
Show References
- Patients with multiple sclerosis (MS), the most common autoimmune, inflammatory, demyelinating neurological condition, often present to the emergency department with their first episode of symptoms and for treatment of future exacerbations.
- While the diagnosis of MS is ultimately made based on clinical findings such as visual abnormalities, sensory and motor complaints, gait abnormalities, and fatigue, use of brain MRI and cerebrospinal fluid (CSF) studies may be helpful in making the diagnosis.
- Brain MRI findings that are suggestive of MS include ovoid-shaped, demyelinated plaques often situated in periventricular regions and near the corpus callosum. Seventy to 95% of MS patients will have an abnormal brain MRI.
- CSF findings suggestive of MS include oligoclonal IgG banding and is discovered in 85 to 95% of cases.
Show References
Beware Trendelenburg Positioning in the Critically Ill Obese Patient
- When inserting a central venous catheter (CVC) into the internal jugular or subclavian vein, clinicians often place patients in the Trendelenburg position to increase the size of the vein.
- When possible, avoid Trendelenburg position for CVC placement in the morbidly obese patient.
- These patients can quickly deteriorate in this position due to reduced lung volumes, increased right heart pressures, decreased cardiopulmonary reserve, and the effects in intra-abdominal pressure.
Show References
In the second half of pregancy, we've traditionally learned that the gravid uterus compresses the inferior vena cava and therefore decreases cardiac output when patient is in a supine position. Therefore, we've learned that patients in the second half of pregnancy the patient should be placed in a left lateral tilt position.
However, it is difficult to perform good quality chest compressions when the patient is in a titled position.
Therefore, the optimal position for chest compressions on the patient in cardiac arrest in the second half of pregnancy is to have the patient in a supine position; and have another rescuer manually deflect the uterus to the patient's left side. This provides optimal compressions + optimal venous return.
Show References
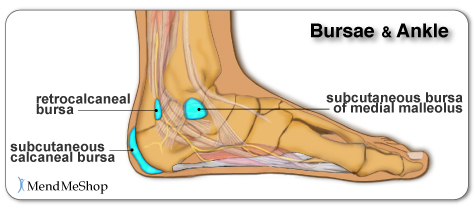
Chief complaint: “Posterior heel pain”
http://www.aidmybursa.com/_img/ankle-retrocalcaneal-subcutaneous-bursitis.jpg
{kind=link}
Retrocalcaneal bursitis
The retrocalcaneal bursa is located between the Achilles tendon and the posterior superior border of the calcaneus.
H&P: Inflammation and pain may follow repetitive dorsi/plantar flexion of the ankle (excessive running, jumping activities). Tenderness anterior and superior to the Achilles insertion on the heel.
Treatment: Minimize weight bearing. ½ inch elevation. NSAIDs.
Posterior calcaneal bursitis
This bursa is subcutaneous, just superficial to the insertion of the Achilles tendon.
H&P: Inflammation and pain may follow irritation from the upper border of the heel counter of a shoe. Posterior heel pain. Tender “bump” (the inflamed and swollen bursa) on the back of the heel.
http://podiatry.files.wordpress.com/2006/12/patient2.jpg
{kind=link}
Treatment: Opened-heeled shoes, sandals, or placement of a “U-shaped” pad between the heel and the counter. NSAIDs. Advance to shoes with soft or less convex heel counters.
Show References
- occurs in 1/1000 live births, but found in 15% of neonatal autopsies
- usually weigh <2500 grams at birth with prematurity the most common risk factor
- present with bleeding from the nose and mouth with severe respiratory distress
- immediate treatment with tracheal suctioning, oxygen, and positive-pressure ventilation
- ventilation goal is to maintain a high, positive expiratory pressure of at least 6-10cm H20
- also check for and correct any underlying bleeding disorders
- extremely high mortality, but no long-term pulmonary deficits if the infant survives
Show References
As we eat our turkey today and the myth that we are tired because of the tryptophan content is propagated further - nothing to do with the 2000kcals that we just ate - I would like to share an interesting and controversial study.
Use of stimulants and and sedatives by EM residents. Incidence is as follows:
In a study of 485 residents with 47% response rate:
Prescription Stimulants: 3.1%
Sleep Aids (all): 89%
Use of Nonbenzodiazepines (zolpidem): 14%
Use of Melatonin: 10%
Benzodiazepines: 9%
Difficult job with difficult hours. What is the appropriate medication or is there a medication that truly assists with performance? Are they doing harm to themselves? to patients?
Disrupted circadian rhythm, addiction tendencies and the hardship of a stressful nightshifts are the price we pay for this specialty. Awareness and education are needed for the residents as well as the attendings.
Show References
- Any patient presenting with an acute onset of dizziness described as a spinning sensation should be thoroughly assessed for cerebellar stroke, as these often present in such a manner, prior to assuming that the source is simple vertigo.
- Cerebellar strokes, whether due to infarct or hemorrhage, typically present with ataxic gait, abnormal Rhomberg, dysmetria with finger-to-nose and heel-to-shin testing, and nystagmus.
- In addition, the dizziness associated with cerebellar strokes should be less reproducible and extinguishable than that due to simple vertigo.
- In terms of imaging, remember that CT scanning is not the preferred radiologic modality for evaluating the cerebellum and posterior aspects of the brain; the thickness of the posterior skull tends to create significant artifact and distortion. If suspicion warrants, MRI should therefore be pursued.