Search
The Prehospital Acute Neurological Treatment and Optimization of Medical Care in Stroke Study (PHANTOM-S) was a randomized prehospital clinical trial. On certain days, a dedicated Stroke Emergency Mobile (STEMO) responded to possible ischemic stroke incidents. Outcomes measured included time to thrombolysis and adverse events such as intracerebral hemorrhage. As opposed to usual prehospital care, a STEMO ambulance was equipped with a CT scanner, point of care laboratory, and a neurologist. According to the study, STEMO use resulted in reduced time to treatment (tPA) without adverse events.
Though this trial did not specifically measure clinical endpoints, it addresses issues central to the delivery of specialized prehospital care:
1) Are there certain conditions which might warrant a tailored, super-specialized EMS response?
2) Are EMS systems capable of delivering definitive care to the patient as opposed to delivering the patient to definitive care?
Stateside study has already started. The Houston Fire Department, in partnership with UTHeath, has already loosed a "Mobile Stroke Unit" on the streets. Like the STEMO, the specialized ambulance will be University hospital based, carry a neurologist, and have the capability to administer tPA.
STEMO pictures courtesy of the "NeuroEMS Blog"
http://www.neuroems.com/2014/05/14/tpa-in-the-truck-results-of-the-phantom-s-trial/
Show References
Currently, no effective reversal agent for new oral anticoagulants (e.g. direct thrombin inhibitor, dabigatran, and factor Xa inhibitors: rivaroxaban and apixaban) exists for emergent management of hemorrhagic complications.
Boehringer Ingelheim, the manufacturer of dabigatran, is developing an antibody fragment (Fab) against dabigatran as a reversal agent.1
A small ex-vivo porcine study demonstrated partial reversal of anticoagulation effects, measured by PT, aPTT, clotting time, clot formation time and maximum clot firmness, of dabigatran by PCC and activated PCC, while dabigatran-Fab achieved complete reversal. Recombinant fVIIa did not reverse the anticoagulation effect of dabigatran.2
Caution should be exercised when interpreting these finding as reversal of laboratory values does not necessarily correlate with clinical effect/outcome. However, dabigatran-Fab holds promise as an effective reversal agent of dabigatran.
Dabigatran-Fab is still under development and is not available/approved for clinical use.
Show References
- The US tends to average about 2-3 cases of rabies in humans per year
- However, around 6,000 animal cases are reported yearly in the US, so the potential for infection is there.
- Most cases are acquired through contact with infected animals: generally bats, foxes, and unvaccinated dogs (this is a huge problem in low- and middle-income countries)
- Of note, in 2013, a human case was reported in Maryland that was acquired through organ transplantation from an infected donor
Clinical Presentation
Rabies is, initially, a clinical diagnosis. To see what a patient with rabies looks like, check out this 3 minute YouTube video: (There is a bit of commentary by the person who posted it at the beginning that you might want to skip through.)
https://www.youtube.com/watch?v=EZbrNN9KeUI
Bottom Line
Rabies, while a rare disease in the US, can occur through either contact with infected animals (especially while traveling) or via organ transplantation. Recognizing the clinical syndrome is key to diagnosis.
University of Maryland Section for Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Show References
Prior literature has demonstrated the safety and feasibility of placing subclavian lines with ultrasound guidance; here's a link to a short educational video describing the technique.
The literature has been varied, however, as to which approach is best for venous cannulation with ultrasound; the supraclavicular (SC) or infraclavicular (IC) approach (see references below)
A recent study evaluated both approaches in healthy volunteers in order to determine which approach is superior for cannulation using ultrasound.
98 patients were prospective evaluated by Emergency Medicine physicians with training in ultrasound. In each patient, both SC and IC views were evaluated on both the left and right sides; each view was given a grade for ease of favorability (no patients were actually cannulated)
Overall, it was found that the SC view was significantly more favorable compared to the IC view; the right SC was non-significantly preferred compared to the left SC.
Show References
Risk Modifiers for Concussion and Prolonged Recovery
A history of prior concussion is a risk factor for future concussion (>2x risk).
For individual sports, boxing has the highest risk.
For team sports, football, ice hockey and rugby have the highest risk.
Women’s soccer confers the highest risk for female athletes.
Younger age confers increased risk.
Female sex confers higher risk when comparing similar sports with similar rules.
Those with migraine headaches may be at increased risk.
Risk of prolonged concussion
Most athletes have symptom resolution within one week
Post traumatic amnesia (both retrograde and anterograde) predict increased number and longer duration of symptoms.
Younger age also predicts pronged recovery.
Other studies have found associations with headache lasting greater than 60 hours, fatigue, “fogginess,” or greater than 3 symptoms at initial presentation. Cognitive studies have identified deficits in visual memory and process speed as predictors of prolonged recovery.
Show References
A placebo-controlled treatment trial in 26 cocaine-addicted subjects aimed to determine whether dexmedetomidine reverses MAP and HR increases after intranasal cocaine (3 mg/kg).
Key Findings
- Low-dose dexmedetomidine (0.4 µg/kg) abolished cocaine-induced increases in MAP (+6 ± 1 versus -5 ± 2 mm Hg; P<0.01), but had no effect on HR (+13 ± 2 versus +9 ± 2 bpm; P=ns).
- Skin sympathetic nerve activity and skin vascular resistance were significantly reduced.
- A higher sedating dose of dexmedetomidine (1.0 μg/kg) was needed to counteract the modest HR rise, but at the expense of increasing BP in one third of patients.
Application to Clinical Practice
In a low nonsedating dose, dexmedetomidine may be a potential (adjunct) treatment for cocaine-induced acute hypertension. However, higher sedating doses can increase blood pressure unpredictably during acute cocaine challenge and should be avoided.
Generous benzodiazepine should remain first-line therapy.
Show References
General Information:
- Previously, polio had been decreasing in incidence and nearing worldwide eradication.
- From 2012 to 2013, the incidence doubled from 223 to 403 cases, and is anticipated to be higher in 2014 (May and June are the highest transmission months).
- The WHO declared a Public Health Emergency of International Concern on Monday (5/5/14).
- Polio has been transmitted across international borders by travelers and is still circulating within endemic areas.
- In addition to improving vaccination within these countries, the public health emergency calls for all travelers from these countries to complete a polio vaccine series and travel with vaccination records.
Relevance to the EM Physician:
- Previously unvaccinated travelers should be given a 3-dose polio vaccine series.
- If a traveler has completed the 3-dose series in the past, the CDC recommends one single lifetime booster dose of inactivated polio virus (IPV).
Bottom Line:
- Polio is increasing in incidence in 10 countries: Syria, Pakistan, Cameroon, Afghanistan, Equatorial Guinea, Ethiopia, Iraq, Israel, Somalia and Nigeria.
- For those who received an IPV series as a child, a single IPV booster is recommended for travelers to those countries to assure lifelong immunity.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD
Show References
High Flow Nasal Cannula
What is it?
- High flow nasal cannula has been used in pediatrics for some time now
- It can be used in adults as well
- It is a simple nasal cannula setup with larger cannula sizes in both nares
- It is heated, humidified oxygen
- You can control your oxygen level and flow of oxygen
Benefits
- Small amount of PEEP provided to the patient (estimated 5-7 cm H20)
- Improves oxygenation (more reliable oxygenation than a non-rebreather face mask)
- Can provide some alveolar recruitment
- Increases FRC (functional residual capacity)
- Pharyngeal dead space washout
Who to use it on
- Acute hypoxemic respiratory failure
- Pre-intubation (can place before and during intubation in patients who have low oxygen saturation)
- Post-extubation
- Palliative care (DNI patients)
How to set it
- Flow rates: 0-60 L/min
- Spontaneously breathing patient with mild-moderate hypoxemia/respiratory distress:
-15-30 L per minute
-100% oxygen (wean as tolerated)
-temp 35-40 C
-when weaning decrease oxygen prior to flow
Bottom line: No evidence that it reduces intubation rates in patients with hypoxemic respiratory failure but may improve oxygenation issues while deciding on treatment options
Show References
Question
The clip below demonstrates normal right femoral anatomy. The structure with the asterisk is the right common femoral vein and the arrow is pointing to a branch of the right femoral vein. What is the name of the branch and what is its importance during lower extremity ultrasound?
Show Answer
Show References
Four small case series (one prospective, 3 retrospective) have concluded that dexmedetomidine (Precedex) may be a useful adjunct therapy to benzodiazepines for ethanol withdrawal in the ED or ICU. They are summarized on the Academic Life in EM blog.
A new randomized, double-blind trial evaluated 24 ICU patients with severe ethanol withdrawal.
Group 1: Lorazepam + placebo
Group 2: Lorazepam + dexmedetomidine (doses of 0.4 mcg/kg/hr and 1.2 mcg/kg/hr).
- 24-hour lorazepam requirements were reduced from 56 mg to 8 mg in the dexmedetomidine group (p=0.037).
- 7-day cumulative lorazepam requirements were similar.
- Clinical Institute Withdrawal Assessment or Riker sedation-agitation scale scores were similar within 24 hours.
- Bradycardia occurred more frequently in the dexmedetomidine group.
Take Home Points
- Dexmedetomidine reduced short-term benzodiazepine requirements, but not long-term when using symptom-triggered approach.
- Monitor for bradycardia when using dexmedetomidine.
Show References
A recent article showed that District of Columbia's Prescription Drug Monitoring program (PDMP) did not change the amount of opioids prescribed after conversion to MMEs (mg morphine equivalents). It is surprising to see a varying effect of PDMPs across the USA. Some have seen dramatic decreases up to 60% in Colorado versus an actual increase of over 50% in Connecticut. Usability, lack of interstate connectivity and quality of information have been seen as rate limiting factors in the efficacy of PDMPs.
PDMPs, by themselves, are not the answer to prescription drug abuse but are an excellent adjunct. Maryland ACEP and a committee chaired by Dr. Suzanne Doyon, Director of the Poison Center, have developed Opioid Prescribing Guidelines and a Discharge pamphlet that can utilized by hospitals to assist with this epidemic. The guidelines and pamphlet have been endorsed by MDPCC, MDACEP, DHMH and a multitude of other Maryland state agencies. I have attached the guidelines.
Show References
Attachments
Background Information:
ACEP has recently revised its 2004 policy on critical issues in the evaluation and management of adult patients with seizures in the emergency department.
Pertinent Study Design and Conclusions:
- A literature review was conducted to derive evidence-based recommendations to help clinicians answer 4 critical questions. Only recomendations relating to question number 4 are presented in this pearl.
- Evidence suggests that in cases refractory to benzodiazepine, valproate works as well as phenytoin and fosphenytoin in status epilepticus as a second-line agent. Compared to phenytoin or fosphenytoin, valproate can be given more quickly and has fewer adverse effects (Level B recommendation).
- This recommendation is intended for adult patients aged 18 years and older presenting to the ED with generalized convulsive seizures.
Bottom Line:
As an alternative to phenytoin or fosphenytoin, valproate may be considered for refractory convulsive status epilepticus if benzodiazepines fail.
University of Maryland Section of Global Emergency Health
Author: Walid Hammad, MB ChB
Show References
Attachments
- 1404301058_ACEP_Clinical_Policy_Neurology_2014.pdf (607 Kb)
- 1404301059_ACEP_Clinical_Policy_Neurology_2004.pdf (217 Kb)
Antibiotic Timing in Severe Sepsis/Septic Shock
- Though the recent ProCESS trial has questioned the utility of central hemodynamic monitoring and protocol-based resuscitation, early antibiotic administration remains paramount in the care of patients with severe sepsis/septic shock.
- Retrospective studies have demonstrated that delays in antibiotic administration are associated with marked increases in hospital mortality.
- Notwithstanding, delays in antibiotic administration remain all too common.
- Ferrer et al, have just published the largest cohort to date analyzing the association of antibiotic timing to hospital mortality in patients with severe sepsis or septic shock. The key findings include:
- Retrospective cohort of 17,990 patients from the SSC database.
- Hospital mortality rose linearly for each hour delay in antibiotic administration.
- Odds ratio for hospital mortality increased from 1 to 1.52, as the delay increased from 0 to 6 hours after presentation.
- Key Point: Antibiotic timing matters!
Show References
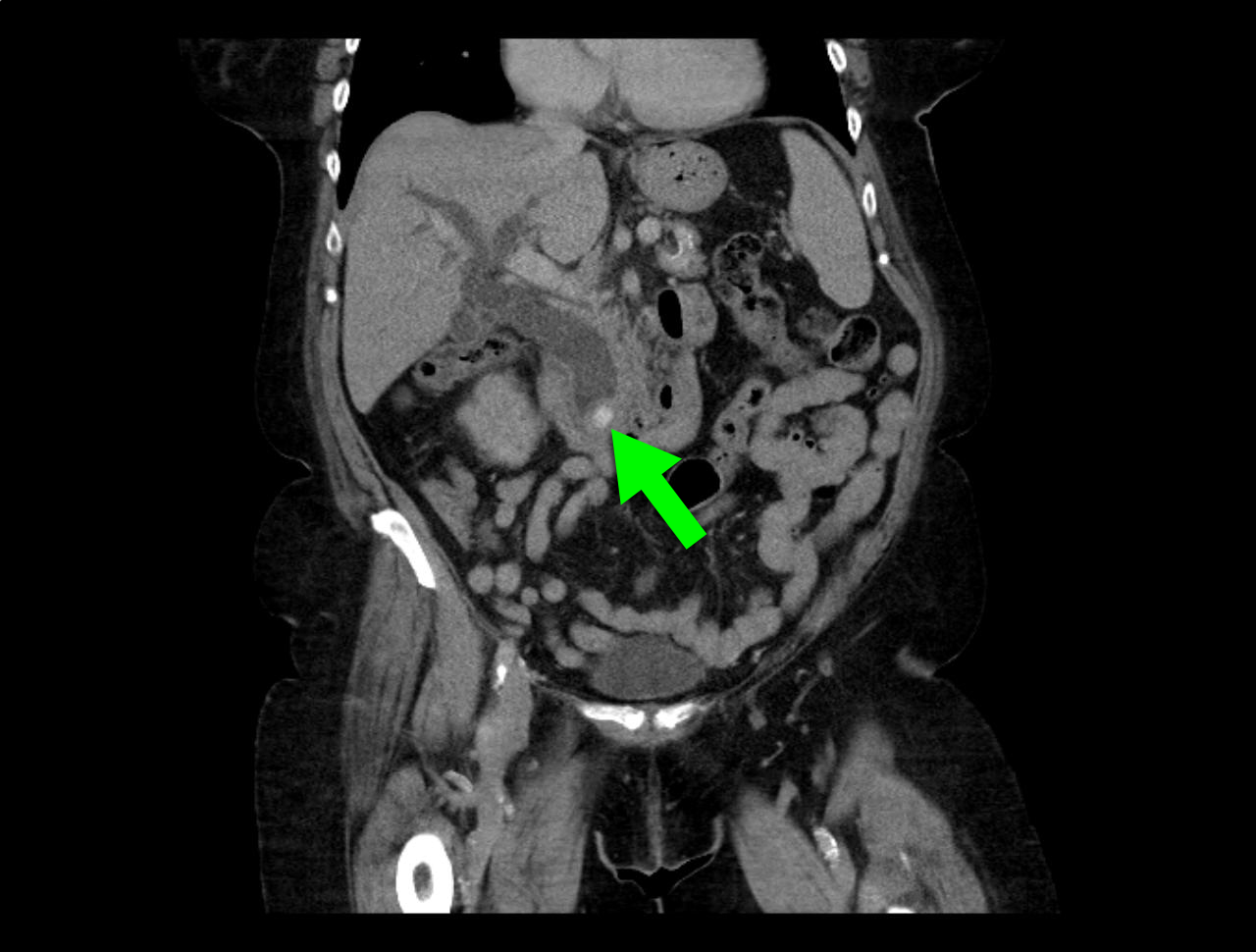
Question
66 year-old female presents with one week of epigastric and right flank pain. Urinalysis was normal. What’s the diagnosis?

Show Answer
Show References
Show References
Acetaminophen spent much of 2013 being chased by paparazzi and sharing magazine covers with Miley Cyrus. What a fall from stardom after becoming known as the pain reliever “hospitals use most,” and the one, “recommended by pediatricians.” Slogans we know well based on $100 million/year spent on advertising.
Approximately 150 patients a year die from unintentional acetaminophen poisoning averaged over the past 10 years. From 2001 to 2010, annual acetaminophen-related deaths amounted to about twice the number attributed to all other over-the-counter pain relievers combined,
The FDA sets the maximum recommended daily dose of acetaminophen at 4 grams, or eight extra strength acetaminophen tablets.
Ingestion of 150 mg/kg or approximately 10g for a 70 mg individual reaches the toxic threshold for a single ingestion. The toxic threshold decreases in cases of chronic ingestion.
Patients who “unintentionally” overdose have been found to take just over 8g per day (almost double the recommended maximum). This is unlikely due to taking one extra 325mg tablet once or twice.
Before we all go on a mad NSAID prescribing binge, let's all be aware of the dangers, educate our patients and allow Acetaminophen to walk the red carpet again.
Show References
Venomous snakes are believed to be everywhere in the United States except Maine, Hawaii, and Alaska. Most snakebites occur from months of April to October since snakes hibernate in the winter. Most bites occur in the extremities (lower > upper). One of the serious clinical manifestation of snakebite is compartment syndrome.
The following are risk factors for the development of increased intracompartmental pressures:
1) Envenomation of small children
2) Envenomation of digits
3) Application of ice or cold packs
4) Delayed use of antivenin
5) Inadequate dosing of antivenin
Show References
General Information:
- Middle East Respiratory Syndrome (MERS) is a viral illness caused by the coronavirus MERS-CoV.
- First reported as a novel species in Saudi Arabia in September 2012, it has an estimated fatality rate of 40%.
- MERS can present like a URI or can be as severe as pneumonia and ARDS.
- More than half of the laboratory-confirmed secondary cases have been associated with health care settings.
Area of the world affected:
- A second spike of cases occurred over the past few weeks in the Arabian Peninsula and has spread to Northern Africa and Europe.
- All cases outside of the Middle East involve patients that have either been to the Middle East or have been in contact with someone returning from the region.
Relevance to the US physician:
- Inbound travel to the US from the Middle East increases significantly between April and September. The WHO’s Global Alert Response recommends that countries with travelers from the Arabian Peninsula maintain a high level of vigilance.
Bottom Line:
Evaluate patients for MERS-CoV infection if they develop fever and pneumonia within 14 days after traveling to countries in or near the Middle East or if they had close contact with someone from this area.
University of Maryland Section of Global Emergency Health
Author: Walid Hammad, MB ChB
Show References
Direct vs. video laryngoscopy in the patient with an acute TBI
Hypoxia and hypotension are considered the "lethal duo" in patients with traumatic brain injury. In a recent randomized control trial (by our own Dr. Dale Yeatts at the Shock Trauma Center) mortality outcomes were compared between 623 consecutive patients who were intubated with either direct laryngoscopy (DL) or video laryngoscopy (VL). Here is what they found:
1. No significant difference in mortality for all comers (Primary Outcome)
2. In the subset of patients with severe head injuries, there was:
- A significantly higher mortality in patients with TBI if VL was used
- A significantly longer intubation duration for VL (74 sec) than DL (65 sec)
- A greater incidence of low oxygen saturations of 80% or less in the VL group (27 patients) than DL (15 patients) - objectively recorded data, not self reported.
There is a reasonable amount of literature that shows hypoxia and hypotension significantly contribute to morbidity & mortality in the TBI patient, and a growing body of literature that suggests intubation with VL takes longer than DL.
Bottom Line: When choosing a method of intubation for the TBI patient, remember the "Lethal Duo" and consider direct laryngoscopy with manual inline stabilization first.
Show References
Subcutaneous Defibrillator
- The implantable cardioverter-defibrillator (ICD) has evolved from devices through epicardial patch electrodes introduced by thoracotomy to transvenous leads advanced to the right ventricle
- Transvenous ICD (T-ICD) reduced the morbidity associated w/thoracotomy implants, however involves potential complications including: hemopericardium, hemothorax, pneumothorax, lead dislodgement, lead malfunction, device-related infection, and venous occlusion
- Subcutaneous ICD (S-ICD) offers the advantage of eliminating the need for intravenous & intracardiac leads. Clinical trials have proven its effectiveness in detecting and treating ventricular fibrillation/tachycardia; however its major disadvantage is its inability to provide bradycardia rate support and anti-tachycardia pacing to terminate ventricular tachycardia
- No study has directly compared the T-ICD & the S-ICD, however clinical data suggests that its use be considered in relatively younger patients (i.e., age <40 years), those at increased risk for bacteremia, patients with indwelling intravascular hardware at risk for endovascular infection, or in patients with compromised venous access