Search
What are characteristics that increase the chance a patient is at risk for opioid-related death? A recent JAMA article begins to tackle this very issues. Baumblatt et al. found the following:
1) Patient with 4 or more prescribers had adjusted odds ratio 6.5 for opioid-related death
2) Patient with 4 or more pharmacies where they get their prescriptions aOR - 6.0
3) Patient with more than 100 mg of morphine equivalents mean per day aOR - 11.2
With the new Maryland Prescription Drug Monitoring program (PDMP) we can start looking at a patient's prescription drug use pattern. The recent JAMA article can help you identify patients at high risk to die an opioid-related death. Use the PDMP and be wary if a patient has more than 4 prescribers or pharmacies or has >100mg of morphine equivalents per day.
Show References
Question
You are evaluating a 40 year old trauma victim and see this on pelvic xray. What are you worried about?

Show Answer
Nitric Oxide appears to have NO role in ARDS
Background: The use of inhaled nitric oxide (iNO) in acute respiratory distress syndrome (ARDS) & severe hypoxemic respiratory failure has been thought to potentially improve oxygenation and clinical outcomes. It is estimated that iNO is used in up to 14% of patients, despite a lack of evidence to show improved outcomes.
Mechanism: Inhaled NO works as a selective pulmonary vasodilator which has been found to improve PaO2/FiO2 by 5-13%, but is costly ($1,500 - $3,000 per day) and increases risk of renal failure in the critically ill.
Study: A recent systematic review analyzed 9 different RCTs (N=1142) and compared mortality between those with severe (PaO2/FiO2 < 100) and less severe (PaO2/FiO2 > 100) ARDS and found that iNO does not reduce mortality in patients with ARDS, regardless of the severity of hypoxemia.
Bottom Line: Inhaled NO is an intriguing option for the treatment of refractory hypoxemic respiratory failure, however there does not appear to be a mortality benefit to justify it's high cost and potentially negative side effects. In the ED, it is important to focus on appropriate lung protective ventilation strategies (TV: 6-8 cc/kg IBW) and maintaining plateau pressures < 30 cm H2O in the initial stages of ARDS to prevent ventilator induced lung injury while awaiting ICU admission.
Show References
The number of patients with left ventricular assist devices (LVADs) is increasing and development of optimal resuscitative strategies is becoming increasingly important. Despite a lack of evidence, many device manufacturers and hospitals have recommended against performing chest compressions because of fear of cannula dislodgment or damage to the outflow conduit.
A recent retrospective analysis of outcomes in LVAD patients who received chest compressions for cardiac arrest did not support the theory that LVADs would be harmed by conventional resuscitation algorithms.
The study was a limited case series of only 8 LVAD patients over a 4 year period. All patients received compressions and device integrity was subsequently assessed by blood flow data from the LVAD control monitor or by examination on autopsy. Although more research is necessary to determine the utility and effectiveness of compressions in this population, none of the patients in this study had cannula dislodgment and half of the patients had return of neurologic function.
Show References
Ankle Syndesmosis Injuries are also called high ankle sprains as they involve trauma to the ligaments above the ankle joint
Most ankle sprains are lateral ankle sprains. High ankle sprains are relatively uncommon.
Usual mechanism: External rotation injuries
Exam: Tenderness at the syndesmosis and compression of the tib/fib at the mid calf level causing syndesmosis pain (squeeze test)
Median recovery time is almost 4 times as long as a lateral ankle sprain 62days vs. 15days
Emergency department care is similar tto that of other ankle sprains but the added benefit of patient education and advice may improve overall care and follow-up.
Show References
Question
35yo M with history of rheumatic heart disease presents with fever. What disease process is suggested by the echo?
.JPG)
Show Answer
Show References
Attachments
In 2001, Rivers et al. published a landmark article demonstrating an early-goal directed protocol of resuscitation that reduced mortality in septic Emergency Department patients.
Many questions have arisen throughout the years with respect to that trial; critics have complained about the overwhelming change in clinical practice based on this one single-center randomized trial.
Challenging Rivers data are the ProCESS (Protocolized Care for Early Septic Shock) investigators, who released the results from a multi-center randomized control trial of 1351 septic Emergency Department patients; the primary end-point was 60-day mortality. Click here for NEJM article.
Patients in this trial were randomized to one of three groups:
-
Protocol-based EGDT
-
Protocol-based standard (did not require central lines, inotropes, or blood transfusions
-
Usual care (no specific protocol; care was left to the bedside clinicians)
Bottom-line: The investigators did not find any difference in mortality between patients in the three groups and comment that the most important aspects of managing the septic patient may be prompt recognition and early treatment with IV fluids and antibiotics.
Show References
Question
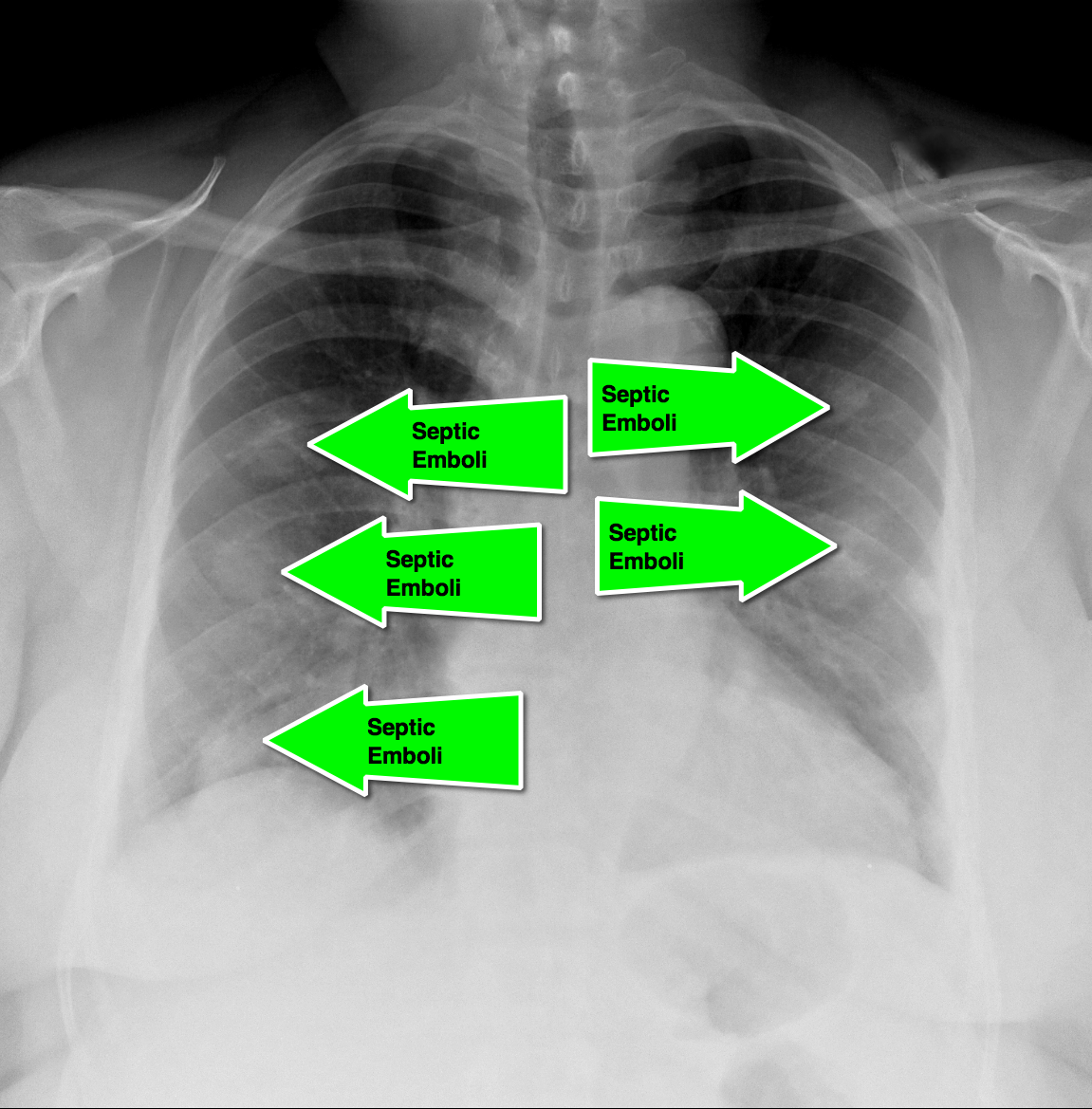
62 year-old male presents with weakness, chills, cough, and malaise. Recently, he had four teeth extracted but felt fine immediately after the extraction. Past medical history includes diabetes and hypertension; CXR is below. What’s the diagnosis?
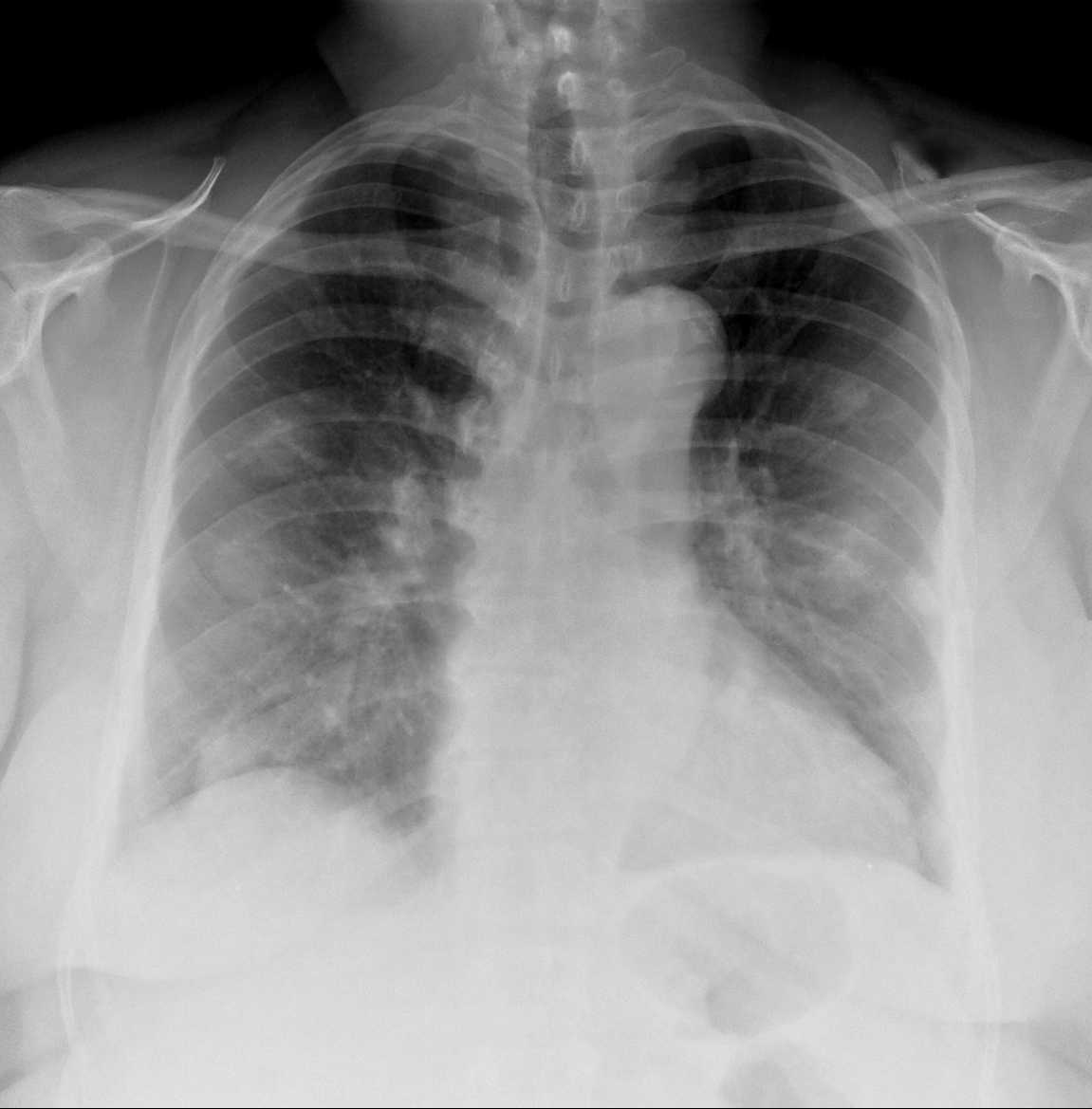
Show Answer
Show References
The HEART Score
Acute coronary syndrome defines a spectrum of diseases (unstable angina, NSTEMI, STEMI), without clear ECG abnormalities the diagnosis and disposition can be challenging
Several scoring systems have attempted to risk stratify patients: TIMI, PURSUIT, and GRACE
The TIMI & PURSUIT scores were designed to identify higher-risk patients and long-term mortality
A pilot/observational study has utilized a novel scoring system to risk stratify low to intermediate risk patients
The HEART (History, ECG, Age, Risk factors and Troponin) score:
- 0-3 points ~ 2.5% risk (data supporting discharge)
- 4-6 points ~20.3% risk (data supporting observation)
- ≥7points ~ 72.7% risk (data supporting early invasive strategies)
This scoring system is limited given the small study size and requires further study/validation, but may be an easy, quick, and reliable predictor of outcome in chest pain patients
Show References
Carbon Monoxide Half-Life:
- Average elimination on room air: 5-6 hours
- 100% Oxygen: 70-130 minutes
- 100% Oxygen under hyperbaric conditions at 3 ATA: 23 minutes
Show References
Question
35 year-old carpet-layer presents with swelling of the superior portion of his knee that has progressively gotten worse over one week. He has no fever and has full range of motion (although pain is worse with movement). The knee is not tender to touch and the area is not erythematous or warm. What's the diagnosis?

Show Answer
Show References
In a collaborative effort between the Illinois Poison Center and the Illinois Hospital Association, a new study sought to determine a poison center's effect on hospital length of stay (LOS) and hospital charges.
While the methodology was understandably complex, the authors compared ~5,000 toxicology inpatients with poison center assistance to 5,000 toxicology inpatients without poison center assistance.
After adjusting for confounders, the LOS among patients with posion center assistance was 0.58 days shorter compared to that of patients without poison center assistance (CI 95%: -0.66, -0.51, p<0.001). Though hospital charges for poison center-assisted patients in the lower quintiles were significantly higher than patients without poison center-assistance (+$953; p<0.001), they were substantially lower in the most costly quintile of patients (-$4852; p<0.001).
Poison center assistance was associated with lower total charges only among the most expensive to treat. However, this outlier group is very important when discussing medical costs.
Show References


- “B-Lines” can be seen in patients with pulmonary edema (see attached image below)
- A “B-line” is a reverberation artifact defined by Lichtenstein as having several properties:
1. A comet-tail artifact
2. Arising from the pleural line
3. Well defined
4. Hyperechoic
5. Long (does not fade)
6. Erases A lines
7. Moves with lung sliding
- A large amount of B-lines is pathologic
- These artifacts are also called “comet-tails” due to their appearance
- One or two B-lines can be seen in dependent lung zones in normal lungs
- AIS (Alveolar interstitial syndrome) describes a group of conditions including pulmonary edema, interstitial pneumonia, and pulmonary fibrosis that show similar findings on lung ultrasonography
- The most common presentation of this syndrome is from cardiogenic pulmonary edema and is characterized by B-lines in multiple lung zones
- B lines correspond with interlobular septal thickening on CT scans, which represent pulmonary vascular congestion
Technique
- B-mode is used with the micro-convex (cardiac) probe scanning in at least 8 lung zones
- Quantify the number of B-lines in each zone
- A lung zone is considered to be “positive” when three or more B-lines are present in a longitudinal plane between two ribs
- Two or more regions bilaterally are required to be defined as AIS
- Bilateral diffuse B-lines have a specificity of 95% and a sensitivity of 97% for the diagnosis of pulmonary edema
Show References
Attachments
Hot off the press! Pediatrics March 2014 just published results of a meta-analysis that compared 1 or 2 dose regimens of Dexamethasone versus 5 day course of Prednisone/Prednisolone for management of acute asthma exacerbations in pediatric patients. The results showed that Dexamethasone was as efficacious as the longer course of Prednisone. End points used were return trips to the emergency department and hospital admissions. On further review of the literature, parents tend to prefer the shorter duration of therapy with Dexamethasone. Also, there is less vomiting associated with Dexamethasone. There have been several articles published that show Dexamethasone is more cost-effective than Prednisone. Bottom line: consider giving single dose of Dexamethasone in the ER and then sending patient home with 1 additional dose.
Show References
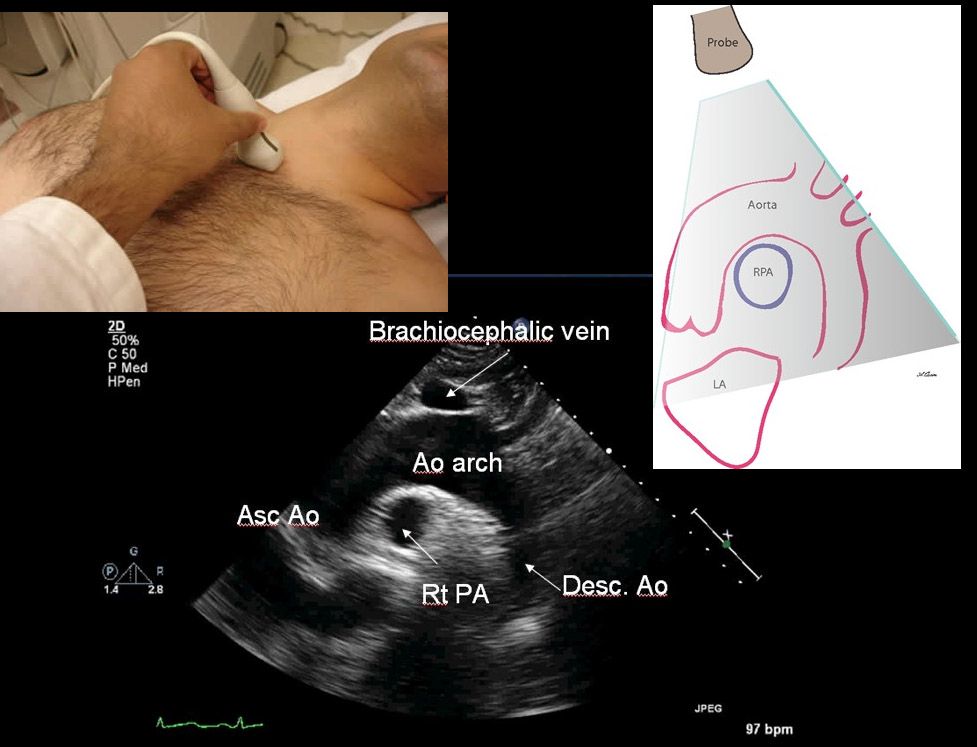
Early diagnosis and surgical consultation for dissection of the ascending aorta can be life saving. Emergency physicians are increasingly using focused cardiac ultrasound to assess chest pain patients in the ED.
The suprasternal notch view (SSNV), may provide additional information in the assessment of thoracic aortic pathology. A recently performed pilot study aimed to determine the accuracy of using the SSNV, in addition to the more traditional parasternal long axis view in assessing aortic dimensions as well as pathology compared to CTA of the chest.
Using a maximal normal thoracic aortic diameter of 40 mm, diagnostic accuracy in detecting dilation of the aorta was 100%. The study showed that the SSNV is feasible and demonstrates high agreement with measurements made on CTA of the chest.
Show References
Herpes Gladiatorum in Wrestlers
HSV causes non genital cutaneous infections primarily in wrestlers, commonly called herpes gladiatorum (HG)
Annual incidence in NCAA wrestlers is 20% to 40%
Most common cutaneous infection leading to lost practice time (40.5% of all infections)
Transmission is skin to skin.
Incubation period is 4 to 7 days from exposure. Healing usually occurs within 10 days after the initial lesion (without scaring).
Appearance: Numerous grouped uncomfortable (painful) vesicles/pustules on an erythematous base…evolve into moist ulcerations, followed by crusted plaques. Lesions typically get abraded during competition therefore may have an atypical appearance and may be mistaken for other infections such as staph. Distribution typically more diffuse than typical HSV infections. Occurs on body surfaces areas that typically come into contract with opponents (face, head, neck, ears, upper extremities). Lesion location typically on side of patient’s handedness. Recurrences occur at location of initial outbreak, a useful diagnostic aid.
Perform a thorough examination as ocular involvement was seen in 8% of high school wrestlers in one HG outbreak.
Typical treatment for primary infection is Valacyclovir 1g PO b.i.d. for 7 days. This is best started within 24h of symptom onset.
Show References
Aseptic meningitis is meningitis with negative bacterial cultures. Overall, viral infections are the most common etiology, however medications can also cause this illness.
Well known causes of aseptic meningitis include: antimicrobials (particularly sulfamethoxazole/trimethoprim), NSAIDS, antivirals (valacyclovir), and antiepileptics.
Recently an abstract was published that suggests that patients on levetiracetam have a higher risk of developing aseptic meningitis than those on topiramate and gabapentin. Lamotrigine has also been implicated, but appears to have a lower risk than levetiracetam, topiramate and gabapentin.
Show References
Case Presentation:
53 yo male presents with fever, myalgia, maculopapular rash, and severe polyarthralgia. He just returned from a cruise to the Caribbean islands.

Clinical Question:
What is the diagnosis?
Answer:
Chikungunya Virus
- Travelers who go to the Caribbean are at risk of getting chikungunya. Cases have been reported in Saint Martin, Martinique, and Guadeloupe. In addition, travelers to Africa, Asia, and islands in the Indian Ocean and Western Pacific are also at risk.
- Mosquito vector, incubation 3-7 days
- Joints involved are typically hands and feet, usually symmetric, severe arthralgia often debilitating
- Dx: serology - ELISA, IgM
- Treatment: IVF, NSAIDS, supportive
Bottom Line:
- Include Chikungunya in your differential of non-specific fever, rash, headache and arthralgia in travelers the Caribbean and endemic areas.
University of Maryland Section of Global Emergency Health
Author: Veronica Pei, MD