Search
Question
Elderly male presents with the skin findings below. He is also on a medication for atrial fibrillation. What's the diagnosis?

Show Answer
Show References
Posterior Myocardial Infarctions (PMI)
- Posterior myocardial infarctions (PMI) are different than typical ST-elevation MI; the ECG findings include: septal & anterior ST-segment depression, dominant tall/broad R waves, and upright T waves.
- In a study among 117,739 subjects with STEMI, 824 with PMI were more likely to present with cardiac arrest, cardiogenic shock, and congestive heart failure.
- The median time from arrival ECG to revascularization with PCI was longer among subjects with PMI.
- The median time from arrival ECG to systemic thrombolysis was also longer among subjects with a PMI.
- Increased awareness and recognition of PMI is needed to improve reperfusion times among this subpopulation with STEMI.
Show References
Overuse injury
Seen in runners, military recruits (marching), ballet dancers and in jumping sports (heavy landing).
Insidious onset of heel pain, that is worse with jumping then running then later with simple weight bearing.
Tenderness to palpation posteriorly (medially or laterally), and squeezing bilateral posterior calcaneus.
Testing:
XR: May not be positive for 2 to 4 weeks. Sclerotic appearance (vertically oriented) posterior calcaneus.
MRI: high signal T2 at fracture site.
DDx: plantar fasciitis.
Treatment: Reduction of activity if Sxs mild, for severe pain start a trial of non weight-bearing (boot or splint with crutches).
Stretching of calf, achilles, plantar fascia.
As noted previously (UMEM Pearl of 1/7/2015), tuberculosis (TB) is a major infectious disease that occurs worldwide. Strains of tuberculosis can be resistant to one or more anti-tuberculosis medications. TB strains resistant to at least one medication have been found in all surveyed countries.
What is multidrug-resistant tuberculosis (MDR TB)?
- A TB organism resistant to at least isoniazid and rifampin
- Two of the most common, potent and standard TB medications
- Primary cause of MDR TB is inappropriate or incorrect usage of TB medications
- In 2013, there were approximately 480,000 cases of MDR TB globally
- Most cases were in India, China and the Russian Federation
- A concerning form of resistant TB is extensively drug resistant TB (XDR TB), which is resistant to multiple anti-tuberculosis medications (see UMEM Pearl from 8/14/2013).
Treatment of MDR TB
- MDR TB can usually be treated and cured with second-line treatments
- Use of second-line treatments tend to be more:
- Difficult to access the medications
- Expensive
- Likely to produce severe adverse reactions
Bottom line:
As noted previously, in your emergency department have a high index of suspicion for TB and MDR TB in patients with an appropriate risk profile.
- Recent travel from appropriate countries
- Most TB cases/deaths are in developing countries
- Individuals infected with HIV.
- Individuals using tobacco
- Increases the risk of infection and death from TB.
- Any age group, including children
- Mostly affects young adults in their productive years
Show References
- Intraosseous (IO) is well-recognized as a venous line for delivering a variety of medications, including vasopressors. However, there is not a wealth of literature to support the use of IOs when administering medications for rapid sequence intubation (RSI).
- This prospective observational study was conducted to determine whether an IO can be used to reliably and rapidly administers medications during RSI in trauma patients.
- Thirty-four trauma patients were enrolled in the study and patients had a variety of traumatic mechanisms; blunt, penetrating, burns, and blast. The primate study outcome was the success rate of first-pass intubations using direct laryngoscopy.
- The authors demonstrated a first pass success rate of 97% with a grade I view on 91% of attempts.
- Bottom-line: This is yet another study demonstrating that when rapid and reliable access is needed, IO is an excellent option for venous access.
Show References
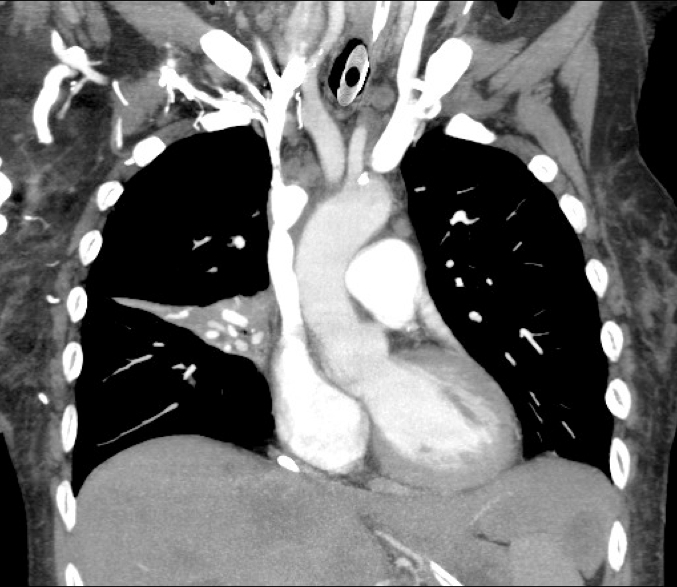
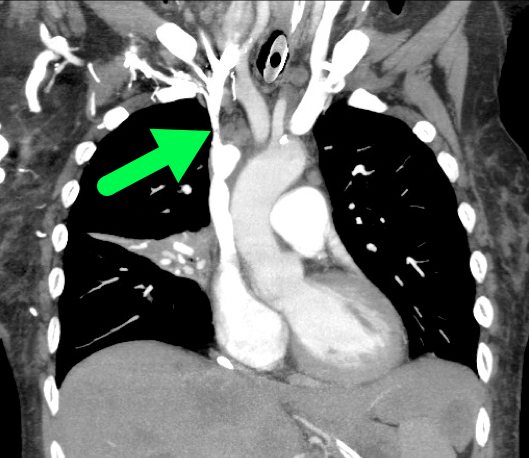
Question
60 year-old male presents with 6 months of weight loss,epistaxis, and increased headache when bending over. What's the diagnosis?
Show Answer
Show References
Of pediatric patients who have anteroposterior (AP) pelvic xrays (XR), there is a 4.6% rate of pelvic fracture or dislocation, compared to 10% in adults.
This study is a sub analysis of a prospective observational cohort of children with blunt torso trauma conducted by PECARN. 7808 patients had pelvic imaging, with 65% of them having an AP XR. The XR sensitivity ranged from 64-82% (based on age groups) for detecting fractures. All but one patient with a pelvic fracture not detected on XR had a CT scan. The CT scan detected all but 2 fractures both of which were picked up later as healing fractures on repeat pelvic XR. Some of the patients who had a missed fracture on XR were hemodynamically unstable or wound up requiring operative intervention.
The authors support the following algorithm:
-With hemodynamically unstability children, obtain a pelvic XR
-For hemodynamically stable children when the physician is planning to get a CT, there is no indication for XR
Bottom line: Consider using AP pelvic radiographs in the hemodynamically stable patient with a high suspicion for fracture or dislocation who are not undergoing CT.
Show References
Left Ventricular Hypertrophy & Arrhythmias: Any Association?
Associations between left ventricular hypertrophy (LVH) and both supraventricular (SVT)/ventricular arrhythmias (VT/VF) have previously been reported.
A recent review & meta-analysis of 10 studies (27,141 patients) revealed the following:
- Incidence of SVT was 11% with LVH compared to 1% without (p <0.001)
- LVH patients had 3.4-fold greater odds of developing SVT
- Incidence of VT/VF was 5.5% with LVH compared to 1.2% without (p <0.001)
- LVH patients has 2.8 greater odds of developing VT/VF
The reason for increased arrhythmogenicity in LVH is not clearly understood.
A consistently observed abnormality in LVH is non-uniform propagation of the action potential throughout the myocardium, which sets the stage for arrhythmias based on early or delayed afterdepolarizations.
Given the heterogeneity in this meta-analysis further research between LVH & sustained arrhythmias is needed to infer true causality.
Show References
We often think of Plantar Fascitis as the cause of heel pain but there are a lot of other causes. Some of those include:
- Heel bursitis- inflammation on the back of the heel. Can be from jumping or poor fitting footwear.
- Heel bumps - from excessively rubbing resulting in too much bone formation.
- Tarsal tunnel syndrome
- Chance inflammation of the heel pad
- Stress fractures
- Severs disease
- Achilles tendonitis
- Retrocalcaneal bursitis
- Posterior calcaneal bursitis
Hydroxocobalamin is an effective cyanide antidote when administered intravenously. Although intraosseous (IO) access is often used in critically ill patients with difficult or delayed IV access, the efficacy of IO administration has not been investigated until recently.
In a recent randomized animal study, acute cyanide toxicity was induced in two groups of swine where 150 mg/kg Hydroxocobalamin was administered via IV vs. IO. The survival rate, reversal of hypotension, and laboratory results were similar between the IV and IO group.
The finding of this study suggest that IO administration of Hydroxocobalamin is as efficacious as IV administration and its administration in acute cyanide toxicity should not be delayed due to lack of IV access when IO access is available.
Show References
Is progesterone yet another disappointing neuroprotectant?
Traumatic brain injury (TBI) affects more than 1.7 million persons in the U.S. annually. The incidence of TBI is increasing globally, especially in developing countries. Despite improvement in trauma systems and critical care, the morbidity and mortality associated with severe TBI remain high.
Progesterone has been shown in preclinical and phase 2 randomized clinical trials to have pluripotent neuroprotective properties and improve mortality in TBI.
Two multicenter phase 3 trials were recently completed and published in the December 25th issue of the New England Journal of Medicine. However, their results were disappointing.
- The Progesterone for the Treatment of Traumatic Brain Injury (PROTECT III) trial, funded by the NIH, looked at progesterone administered within 4 hours after injury in patients with moderate to severe TBI.
- The Study of a Neuroprotective Agent, Progesterone, in Severe Traumatic Brain Injury (SYNAPSE) trial, funded by BHR Pharma, looked at progesterone administered within 8 hours after injury in patients with severe TBI.
Both studies used the Glasgow Outcome Scale (GOS) or Extended Glasgow Outcome Scale (GOS-E) at 6 months as their primary outcome. The GOS and GOS-E capture the degree of recovery from brain injury in terms of disability, stratified into levels by death, vegetative state, severe disability, moderate disability, and good recovery.
Progesterone was not found to have any benefit in functional outcome at 6 months.
Both of these studies were well designed and conducted. However, they were based on small effect sizes of the phase 2 trials. In addition, they had very favorable outcome rates in the placebo group, thereby making it hard to demonstrate a benefit by their sample sizes.
There has been a long history of failed neuroprotectant trials likely due to the complex and variable injury mechanisms involved in TBI. The currently available outcome measures are also insensitive to the targeted mechanistic endpoints. More research is needed to understand not only potential therapies but also how to select appropriate patients for these therapies.
Take Home Point: Progesterone does not have any clear benefit in TBI at this time.
Show References
Diaphragm weakness and its significance
- Acute respiratory failure is partially due to respiratory muscles inability to meet the demands of respiration that is strained by a medical condition
- Ventilation can have an adverse effect on respiratory muscles even after just 5-6 days (atrophy)
There are several ways to monitor diaphragm strength and function
- Airway pressure and flow waveforms
- Occlusion pressure
- Esophageal pressure waveforms
- Sniff maneuvers
- Ultrasound
- Diaphragm EMG
- Chest xray
Clinical Relevance
- Goal is to use these devices to limit the development of respiratory muscle atrophy because of disuse
- Prevent "overassist" from the ventilator
- Potential use in weaning trials to evaluate for respiratory muscle performance
- This is a new area of intensive care research that could lead to improvements in outcomes
Show References
Question
60 year-old male presents with rhinorrhea, body aches, and dry cough for two days. He recently moved here from Kentucky. What’s the diagnosis (please note that there are several differentials based on CXR)?

Show Answer
APACHE-HF Scoring System
The Acute Physiology and Chronic Health Evaluation (APACHE) scoring system was established in the 1980's to predict critically ill patient prognosis (APACHE II, III, and IV have been published in last two decades).
The APACHE II scoring system involves combining 3 separate scores (acute physiology score, chronic health score, and age), which can be cumbersome to apply & thus is not often utilized in the emergency department (modified APACHE II doesn't include chronic health score & is less taxing).
No unique scoring system for acute heart failure (AHF) has been analyzed until present; the APACHE-HF score includes 8 criteria: mean arterial pressure (MAP), pulse, sodium, potassium, hematocrit, creatinine, age, and glasgow coma score (GCS).
AHF in-hospital mortality data was analyzed and compared using APACHE II, modified APACHE II, and APACHE- HF scores and the predictive value of the APACHE-HF score was found to be optimal when compared to the others.
Show References
Mechanism: Direct blow to anterior thigh (Football/basketball) or from a ball traveling at a high rate of speed (field hockey/lacrosse).
Exam: focal tenderness and edema. Pain may be severe and worse with active contraction and passive stretch. Hematoma may already be present. Amount of passive knee flexion at 24 hours can be a clue to the severity of the hematoma.
Treatment: Crutches if pain with weight-bearing. Ice. Immobilization in 120 degrees of flexion immediately after the injury for the first 24 hours may be beneficial.
-Bandage entire lower limb. Provide crutches and pain medication. Soft tissue therapy is contraindicated for the first 48 hours and when instituted must be gentle and cause no pain. Risk of re-bleeding is greatest in first 7 to 10 days.
http://fce-study.netdna-ssl.com/2/images/upload-flashcards/75/20/63/5752063_m.jpg
- Ketamine popularity for procedural sedation is on the rise, again. It provides pain relief, sedation, and memory loss while maintaining airway reflexes and has little effect on the heart.
- Traditional administration has been the intravenous or intramuscular route, but consider intransal now.
- Recent articles have touted the intranasal administration of ketamine for pediatric procedural sedation with good success.
- Admittedly, the number of patients enrolled in the studies to date have been small and the dosages have varied from 1 to 9 mg/kg/dose. However, none of the studies have reported any bad outcomes or complications.
- So, consider IN ketamine for your next pediatric procedural sedation.
Show References
- Potentially toxic ingestions of sustained-release or enteric-coated drugs
- Substantial ingestions of iron, lithium, or potassium
- Removal of ingested packets of illicit drugs in "body packers"
Application to Clinical Practice
WBI can facilitate removal of select toxicants from the gastrointestinal tract in some patients, but there is no convincing evidence from clinical studies that it improves the outcome of poisoned patients.
Show References
Tuberculosis (TB) is a major infectious disease that occurs worldwide.
- TB is second only to HIV/AIDS for the number of individuals killed worldwide from a single agent.
- In 2013, 1.5 million died from TB and 9 million became ill
- The vast majority (>95%) of TB deaths occur in low- and middle-income countries
Fortunately, public health and clinical measures have had some success.
- The estimated number of individuals annually become ill with TB is declining
- The TB death rate dropped 45% between 1990 and 2014
- An estimated 37 million lives were saved between 2000 and 2013 through diagnosis and treatment
Bottom line:
- Tuberculosis (TB) is a major killer worldwide.
- Treatments are available to treat both latent and active disease
- See: http://www.cdc.gov/tb/topic/treatment/
- Good clinical awareness is key to disease identification
Show References
"PQRST" - Capnography in Cardiac Arrest
- Resuscitation of the patient in cardiac arrest can be stressful, chaotic, and variable depending on the setting.
- Capnography is a valuable tool in the management of patients in cardiac arrest.
- Heradstveit, et al. published a pneumonic for the use of capnography during cardiac arrest:
- P - Position of the tube
- The sensivity and specificity of capnography for endotracheal tube confirmation is superior to auscultation and capnometry.
- Q - Quality of CPR
- Early detection of poor-quality compressions.
- R - ROSC
- A sudden increase in end-tidal CO2 can indicate ROSC without interrupting CPR for pulse checks.
- S - Strategy
- May assist clinicians in determining underlying etiology of cardiac arrest.
- T - Termination
- An end-tidal CO2 value < 10 mm Hg after 20 min of resuscitation has been shown to be very accurate in predicting death.
- P - Position of the tube
Show References
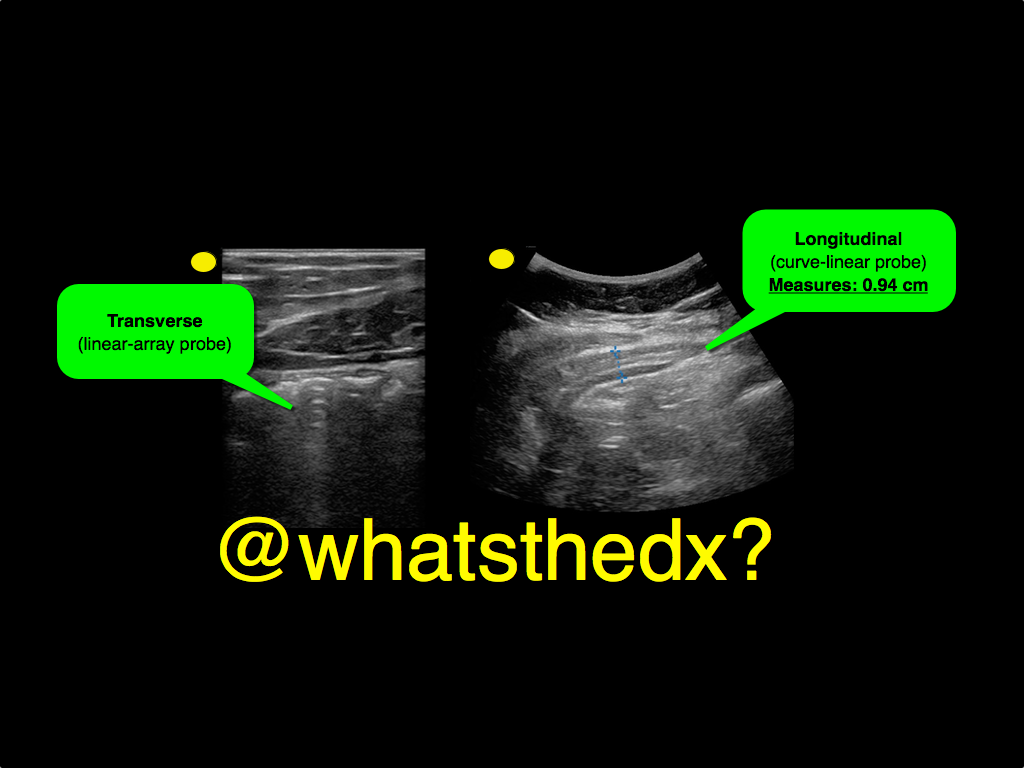
Question
A male patient presents with right lower quadrant pain. The ultrasound is shown at the point of maximal tenderness. The diameter of the structure (image on right) is about 0.94cm. What is this structure and what's the diagnosis?