Search
Refractory Anaphylaxis
- Refractory anaphylaxis is defined as anaphylaxis that does not respond to at least 2 doses of 300 mcg of epinephrine given IM into the anterolateral thigh.
- Refractory anaphylaxis can be due to several factors including patient comorbidities, delayed diagnosis, delayed epinephrine administration, or concomitant beta-blocker or ACE-inhibitor medication use.
- Consider the following treatments in patients with refractory anaphylaxis, persistent hypotension, and shock:
- Aggressive IVF resuscitation - patients may need up to 7L of IVFs
- Epinephrine infusion (1-10 mcg/min) to target a MAP of 65 mm Hg
- Glucagon (1-5 mg via slow IV push) for those taking a beta-blocker and who fail to respond to epinephrine
- Norepinephrine, vasopressin, angiotensin II, methylene blue, or dobutamine can be administered with epinephrine for persistent hypotension.
- VA-ECMO - though there is no prospective evidence on the use of ECMO in anaphylaxis.
Show References
A recent article in Pediatrics attempted to estimate the association between fluoroquinolone use and tendon injury in an adolescent population.
Fluoroquinolones are thought to negatively impact tendons and cartilage in the load-bearing joints of the lower limbs through collagen degradation, necrosis, and disruption of the extracellular matrix.
Population: 4.4 million adolescents aged 12–18 years with filled outpatient fluoroquinolone prescription vs. an oral broad-spectrum antibiotic for comparison.
Fluoroquinolones included ciprofloxacin, levofloxacin, moxifloxacin, and gatifloxacin
Comparator antibiotics included amoxicillin-clavulanate, azithromycin, cefalexin, cefixime, cefdinir, nitrofurantoin, and bactrim.
Outcomes: Primary outcome was 90-day tendon rupture (Achilles, patellar, quadricep, patellar, tibial) identified by diagnosis and procedure codes. Secondary outcome was tendinitis.
Results: The weighted 90-day tendon rupture risk was 13.6 per 100 000 fluoroquinolone-treated adolescents and 11.6 per 100 000 comparator-treated adolescents.
Fluoroquinolone-associated excess risk: 1.9 per 100 000 adolescents; the corresponding number needed to treat to harm was 52 632.
The weighted 90-day tendinitis risk was 200.8 per 100 000 fluoroquinolone-treated adolescents and 178.1 per 100 000 comparator-treated adolescents
Fluoroquinolone-associated excess risk excess risk: 22.7 per 100 000 adolescents; the corresponding number needed to treat to harm was 4405.
Conclusion:
The excess risk of tendon rupture associated with fluoroquinolone treatment was extremely small, and these events were rare. On average, 50,000 adolescents would need to be treated with a fluoroquinolone for 1 additional tendon rupture to occur
The excess risk of tendinitis associated with fluoroquinolone treatment though larger was also small.
Besides tendon rupture, other more common potential adverse drug effects may be more important to consider for treatment decision-making, in adolescents without other risk factors for tendon injury.
Show References
During cardiac arrest, metabolic acidosis develops because of hypoxia-induced anaerobic metabolism and decreased acid excretion caused by inadequate renal perfusion. Sodium bicarbonate (SB) administration was considered as a buffer therapy to correct metabolic acidosis. However, SB has several side effects such as hypernatremia, metabolic alkalosis, hypocalcemia, hypercapnia, impairment of tissue oxygenation, intracellular acidosis, hyperosmolarity, and increased lactate production. The 2010 Pediatric Advanced Life Support (PALS) guideline stated that routine administration of SB was not recommended for cardiac arrest except in special resuscitation situations, such as hyperkalemia or certain toxidromes. An evidence update was conducted in the 2020 Pediatric Life Support (PLS) guideline and the recommendations of 2010 remain valid. This article was a systematic review and meta-analysis of observational studies of pediatric in hospital cardiac arrests. The primary outcome was the rate of survival to hospital discharge after in hospital cardiac arrests. The secondary outcomes were the 24-hour survival rate and neurological outcomes.
Show References
- Post-lumbar puncture (LP) headache, reported in up to 33% of patients, is due to a persistent CSF leak causing intracranial hypotension.
- A recent review by Cognat et al. looked to answer several frequently asked clinical questions:
- Who is at decreased risk of post-LP headache?
- Infants and children have a similar prevalence compared to adults.
- Older patients have a lower risk, with an incidence of <5% in those over 60 years old.
- Does needle choice minimize the risk of post-LP headache?
- Atraumatic non-cutting ("Whiteacre" or "Sprotte") needles have lower rates (RR 0.4, 0.34-0.47).
- The use of atraumatic needles does not affect the rate of success, success on first attempt, or duration of the LP.
- Does performing the LP in a specific way prevent post-LP headache?
- LPs performed in the lateral decubitus position and at a higher intervertebral space have a lower incidence.
- Difficult LPs (e.g. multiple attempts, traumatic tap) do not appear to affect the rate.
- The volume of CSF removed does not affect the rate.
- Do any treatments after the LP reduce post-LP headache occurrence?
- Bed rest after LP does not reduce and may in fact worsen the likelihood.
- Fluids and caffeine do not prevent post-LP headaches.
- Who is at decreased risk of post-LP headache?
Bottom Line: The use of atraumatic needles is most effective in reducing the risk of post-LP headaches. These needles are easy to use and have similar rate of success as cutting needles.
Show References
RECAP: RECOVERY trial is a large, randomized, open label, adaptive trial studying different treatments on COVID-19. Most well known is the use of dexamethasone which reduced mortality by 1/3 in COVID patients requiring mechanical ventilation and by 1/5 in those requiring oxygen, with no benefit on those patients not requiring oxygen.
They recently published results in the Lancet on the use of tocilizumab.
Population:
- Up to 21 days after main randomization, regardless of treatment, RECOVERY trial patients with progressive COVID-19 were eligible for tocilizumab.
Inclusion:
- April 23rd 2020 to Jan 24th 2021-- 21,550 patients with hypoxia (<92% on RA or requiring O2), systemic inflammation (CRP > 75 mg/L) eligible for standard care or standard care plus toci 400-800 mg (dosing based on weight), second dose 12-24 hours later if no improvement
Outcomes:
- Primary outcome 28 day mortality followed by:
- Hospital discharge within 28 days
- Rate of mechanical ventilation
Results:
- 621 (31%) tocilizumab patients and 729 (35%) of usual care patients died within 21 days (RR 0.85, p=0.0028). Consistent even in those receiving steroids (83%).
- Tocilizumab group more likely to be discharged from the hospital, less likely to receive invasive mechanical ventilation (35% vs 42%).
Conclusion:
- Tocilizumab improved survival and other clinical outcomes- by 1/3 for those on simple oxygen, and by ½ for those receiving invasive mechanical ventilation.
- Added to the additional benefit of steroids.
- Findings support the earlier REMAP-CAP trial on the effectiveness of tocilizumab for ICU COVID patients
Show Additional Information
Show References
Both erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are highly sensitive (84-100%) for spinal infections and are observed in >80% with vertebral osteomyelitis and epidural abscesses.
ESR
Most sensitive and specific serum marker, usually elevated in both spinal epidural abscess (SEA) and vertebral osteomyelitis.
ESR was elevated in 94-100% of patients with SEA vs. only 33% of non-SEA patients
Mean ESR in patients with SEA was significantly elevated (51-77mm/hour)
CRP
Not highly specific
Less useful for acute diagnosis since CRP levels rise faster and return to baseline faster than ESR (elevated CRP seen in 87% of patients with SEA as well as in 50% of patients with spine pain not due to a SEA)
Better used as a marker of response to treatment.
Show References
Background:
Cardiac arrest from massive pulmonary embolism (PE) can be up to 90% (1). A recent systemic review evaluated the efficacy of Venoarterial-Extracorporeal Membrane Oxygenation (VA-ECMO) for PE-related cardiac arrest.
Results:
The authors screened 1115 articles and included 77 articles, including gray literature. The authors performed a quantitative analysis of a total of 301 patients.
Overall, 183/301 (61%) patients survived to hospital discharge, a significant improvement from 90%.
Patients who were cannulated during chest compression were associated with 7x higher odds of death (OR, 6.84; 95% CI, 1.53–30.58; p = 0.01), compared to those who were cannulated after ROSC. However, cannulation in the ED was not associated with improved outcomes, compared with other cannulation site.
No increased risk of death among patients who received tPA prior to VA-ECMO vs. those who did not (OR, 0.78; 95% CI, 0.39–1.54; p = 0.48).
Patients whose age > 65 years of age were associated with 3X risk of death, compared to those with age < 65 years (OR, 3.56; 95% CI, 1.29–9.87; p = 0.02).
Take-home points
Please consider “early” VA-ECMO for eligible patients who have cardiac arrest from massive PE. However, it will take great convincing to push the PERT team to cannulate for VA-ECMO while the patient is still receiving chest compression.
Show References
Background:
Cardiac arrest from massive pulmonary embolism (PE) can be up to 90% (1). A recent systemic review evaluated the efficacy of Venoarterial-Extracorporeal Membrane Oxygenation (VA-ECMO) for PE-related cardiac arrest.
Results:
The authors screened 1115 articles and included 77 articles, including gray literature. The authors performed a quantitative analysis of a total of 301 patients.
Overall, 183/301 (61%) patients survived to hospital discharge, a significant improvement from 90%.
Patients who were cannulated during chest compression were associated with 7x higher odds of death (OR, 6.84; 95% CI, 1.53–30.58; p = 0.01), compared to those who were cannulated after ROSC. However, cannulation in the ED was not associated with improved outcomes, compared with other cannulation sites.
No increased risk of death among patients who received tPA prior to VA-ECMO vs. those who did not (OR, 0.78; 95% CI, 0.39–1.54; p = 0.48).
Patients whose age > 65 years of age were associated with 3X risk of death, compared to those with age < 65 years (OR, 3.56; 95% CI, 1.29–9.87; p = 0.02).
Take-home points
Please consider “early” VA-ECMO for eligible patients who have cardiac arrest from massive PE. However, it will take great convincing to push the PERT team to cannulate for VA-ECMO while the patient is still receiving chest compression.
Show References
- Electronic cigarette (E-cigs) smoking (vaping) continues to be a major concern among adolescents and teens, who mistakenly think it is safer than smoking traditional cigarettes or don't consider it as smoking at all.
- Typically, they contain nicotine which is highly addictive and can cause harm in the developing brain, but can also contain other dangerous chemicals, flavorings and drugs.
- They often contain higher amounts and concentrations of nicotine. 1 JUUL pod can contain the equivalent of 20 packs of nicotine cigarettes.
- Inhaled aerosols of the various chemicals, flavorings, and heavy metals have resulted in lung disease and acute respiratory failure. Bilateral infiltrates on chest imaging is a common finding.
- Nicotine toxicity can also occur. Symptoms include vomiting, diarrhea, abdominal pain, salivation, headache, dizziness, confusion, and seizures. Hypertension and tachycardia acutely, followed by hypotension and bradycardia can be expected.
- Bottom Line: Ask specifically about electronic cigarette use in adolescents and teens who present with acute complaints. One study found that of those who regularly used and presented for evaluation of symptoms, 98% were respiratory, 81% were gastrointestinal, and 100% were constitutional in nature.
Show References
- Functional neurological disorders (FND) are unintentional and involuntary.
- Imaging and electrophysiological studies have shown cerebral dysfunctions in attention and perception, which may explain why symptoms often improve with distraction.
- Diagnosis requires demonstration of inconsistency and/or incongruency with recognized neurological or medical conditions.
- No clinical sign alone is diagnostic.
- Patients may have comorbidities such as multiple sclerosis, stroke, or epilepsy.
- Hoover’s sign and drift without pronation have been described as positive signs for FND.
- These can also be seen in patients with pain, neglect, or apraxia.
- Avoid maneuvers that may harm the patient, such as dropping their arm onto their face.
- A high-pitched tuning fork applied to the nostrils is an effective stimulus to assess responsiveness.
- Avoid using terms like non-organic, psychogenic, or pseudoseizure.
- When counseling a patient, avoid only explaining what conditions they do not have or attributing symptoms to psychological problems or stress.
- Instead, name the diagnosis, explain that their symptoms are real and common, and emphasize that symptoms are potentially reversible.
- Early diagnosis of FND is associated with improved physical and psychological outcomes.
Bottom Line: Functional neurological disorders (FND) are commonly encountered in the ED. A thorough neurological exam may reveal positive signs suggestive of FND. Early diagnosis and referral to specialists may improve outcomes.
Show References
Erythrocyte sedimentation rate (ESR) for spinal infection
Sensitive for spinal infection but not specific
Elevated ESR is observed in greater than 80% of patients with vertebral osteomyelitis and epidural abscess
ESR is the most sensitive and specific serum marker for spinal infection
Usually elevated in acute presentations of SEA and vertebral osteomyelitis
ESR was elevated in 94-100% of patients with SEA vs. only 33% of non-SEA patients
Mean ESR in patients with SEA was significantly elevated (51-77mm/hour)
Infection is unlikely in patients with an ESR less than 20 mm/h.
Incorporating ESR into an ED decision guideline may improve diagnostic delays and help distinguish patients in whom MRI may be performed on a non-emergent basis
Show References
Supplemental oxygen therapy is frequently required for patients presenting with acute respiratory distress and COPD exacerbation. Over-oxygenation can derail compensatory physiologic responses to hypoxia,1 resulting in worsening VQ mismatch and, to a lesser degree, decreases in minute ventilation, that cause worsened respiratory failure.
The 2012 DECAF (Dyspnea, Eosinopenia, Consolidation, Acidaemia, and Atrial Fibrillation) score was found to predict risk of in-hospital mortality in patients admitted with acute COPD exacerbation.2,3 Data from the DECAF study’s derivation and external validation cohorts were examined specifically to look at outcome associated with varying levels of oxygen saturation.
- 1027 patients from 6 UK hospitals receiving supplemental oxygen at admission
- Lowest in-hospital mortality seen in the 88-92% cohort
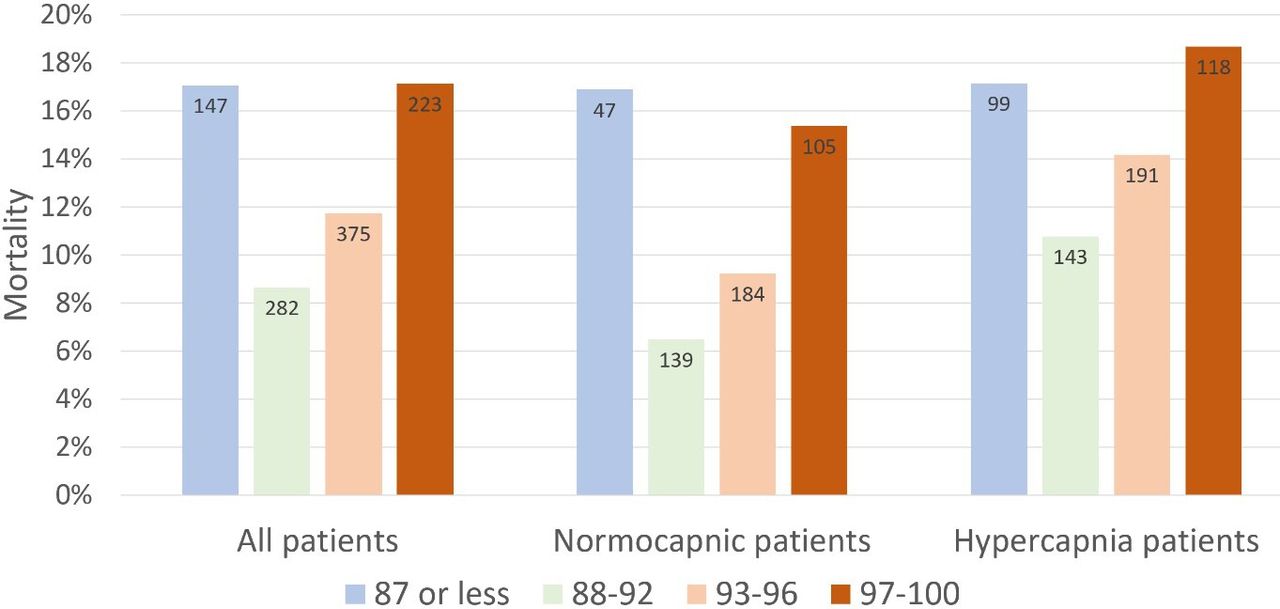
- Adj OR for in-hospital mortality in ≥97% vs 88-92% group: 2.97 (95% CI 1.58-5.58, p=0.001)
- Adj OR for in-hospital mortality in 93-96% vs 88-92% group: 1.98 (95% CI 1.09-3.60, p=0.025)
- Surprisingly, mortality risk seen more in normocapnic than hypercapnic patients
- Association between admission SpO2 and mortality persisted after adjusting for baseline risk and disease severity using the DECAF and NEWS 2 score
Bottom Line
In patients presenting to the ED with acute COPD exacerbation requiring oxygen supplementation, a target oxygen saturation of 88-92% is associated with the lowest in-hospital mortality, and higher oxygen saturations should be avoided independent of patients' PCO2 levels.
Show References
Show References
- Alteplase administration in acute ischemic stroke (AIS) has been associated with errors.
- A recent study looked at the types of errors that occurred at regional hospitals and Comprehensive Stroke Centers.
- 19.8% (133/676) of patients had an error associated with alteplase administration with the majority occurring at regional hospitals without stroke certification.
- The most common error was over-dosage of alteplase, occurring in 5% (36) of patients.
- Other common errors included under-dosage, infusion errors, and apparent contraindications.
- The most common contributing factor leading to the error was incorrect calculation.
- Administration error was associated with higher rate of hemorrhagic conversion (12.7% vs. 7.1%, p=0.04).
Bottom Line: Alteplase administration in acute ischemic stroke is associated with errors, most commonly with over-dosage of the medication.
Show References
Study Question: A recent study investigated whether adult patients presenting to the ED with a diagnosis of mTBI prescribed light exercise were less likely to develop persistent postconcussion symptoms.
Setting: Randomized controlled trial conducted in three Canadian EDs. Consecutive, adults (18–64 years) seen in ED with a mTBI sustained within the preceding 48 hours.
The intervention group received discharge instructions prescribing 30 minutes of daily light exercise.
The control group was given standard mTBI instructions advising gradual return to exercise following symptom resolution.
Outcome: The primary outcome was the proportion of patients with postconcussion symptoms at 30 days,
A total of 367 patients were enrolled. Median age was 32 years Male 43%/Female 57%.
Result: There was no difference in the proportion of patients with postconcussion symptoms at 30 days. There were no differences in median change of concussion testing scores, median number of return PCP visits, median number of missed school or work days, or unplanned return ED visits within 30 days. Participants in the control group reported fewer minutes of light exercise at 7 days (30 vs 35).
Conclusion
Prescribing light exercise for acute mTBI, demonstrated no differences in recovery or health care utilization outcomes.
Extrapolating from studies in the athletic population, there may be a patient benefit for light exercise prescription.
Make sure that the patient is only exercising to their symptomatic threshold as we recommend with concussed athletes. Previous studies have shown that athletes with the highest post injury activity levels had poorer visual memory and reaction time scores than those with moderate activity levels.
Show References
There are three commonly household spices that can be abuse/misused or cause toxicity after exposure.
Pure vanilla extract contains at least 35% ethanol by volume per US Food and Drug Administration standards
- Results in alcohol intoxication
- Ingestion of 1.3 mL/kg in child will result in blood ethanol concentration of 100 mg/dL
Nutmeg contains myristicin – serotonergic agonist that possess psychomimetic properties.
- Typical recreational dose: 5-30 gm. (tablespoon of ground nutmeg: 7 gm).
Clinical effects:
- GI symptoms: nausea, vomiting and abdominal pain
- Cardiovascular: hypertension and tachycardia
- CNS: hallucination, paranoia, seizure
- Others: flushing, mydriasis
Cinnamon contains cinnamaldehyde and eugenol – local irritants.
- Can cause contact dermatitis and ulceration from topical application
- Inhalation of cinnamon can result in chronic and significant pulmonary inflammation and fibrosis
Show References
Two items from the recent INSPIRATION trial UMEM pearl were very well pointed out by our own Dr. Michael Scott and require clarification. Thank you to all our readers for their close attention, and please know that we always appreciate you reaching out with questions/comments.
- Dosing Correction - The "standard-dose" prophylactic dosing of enoxaparin in this trial was 40 milligrams/day. Please excuse the error in the prior post stating 40 mg/kg/day (we will revise the post). Standard dosing of enoxaparin for DVT/VTE prophylaxis was a flat 40 mg/day, and was not weight based.
- Major Bleeding - While the difference in major bleeding (2.5% vs 1.4%) was relatively small, this endpoint DID NOT meet non-inferiority. In other words, the study appeared to detect a statistically significant difference in major bleeding between the dosing regimens. Given that this is a single study and there are concerns with this finding (the authors themselves describe this as "exploratory"), I would interpret this with caution, but this supports the very intuitive notion that the intermediate (higher) dose regimen of enoxaparin would be associated with more bleeding than the standard dose regimen.
COVID-19 is generally regarded as a hypercoagulable state, and the role of pulmonary emboli and other VTE in COVID remains unclear. As a result, how to optimally provide prophylactic anticoagulation in COVID-19 patients who are not known to have VTE has been a point of debate.
The INSPIRATION trial looked at 600 patients admitted to academic ICUs in Iran, and compared what is often-referred to as "intermediate-dose" prophylaxis (in this case 1 mg/kg daily of enoxaparin) to standard dose prophylaxis (40 mg/day of enoxaparin). The study utilized a combined endpoint of venous thromboembolism, arterial thromboembolism, need for ECMO, or mortality. As a reminder, composite endpoints can skew results. However, the dose and type of anticoagulant chosen is similar to many academic centers around the world, and pharmacy guidelines often recommend providing this type of "intermediate-dose" prophylaxis in COVID-19 patients, sometimes based on clinical status, d-dimer or other coagulation-related patient-data. As with many things with COVID-19, this practice is based on limited data.
There was no significant difference between groups in the primary outcome (45.7% in intermediate ppx group vs 44.1% in standard group), and while safety outcomes were similar (major bleeding in 2.5% in the intermediate ppx group vs 1.4% in standard group), the intermediate regimen failed to demonstrate non-inferiority to the standard regimen for major bleeding.
Intermediate vs standard-dose ppx was similar in this study with a small, but statistically significant increase in major bleeding in the intermediate-dose group.
Bottom Line: Although this study had methodologic flaws and there are external validity concerns, the INSPIRATION trial supports the notion that standard dose (e.g. 40 mg/g/kg/day enoxaparin) and intermediate-dose (e.g. 1 mg/kg/day enoxaparin) VTE prophylaxis are equivalent in critically ill COVID-19 patients who do not already have a known VTE in terms of preventing negative VTE outcomes. Intermediate-dose may be associated with increased bleeding. As more critically ill patients require ED boarding, the dose of VTE prophylaxis may remain controversial, but the need to start it remains an important consideration.
Show References
While fluoroquinolones have fallen out of favor for many indications due to the ever growing list of adverse effects, they still play an important role in the outpatient treatment of pyelonephritis. Fluoroquinolones and TMP-SMX are the preferred agents due to higher failure rates with beta-lactams.
Preferred Therapies:
Ciprofloxacin 500 mg PO BID*
Levofloxacin 750 mg PO daily*
TMP-SMX 1 DS tab PO BID**
*Consider a single dose of long-acting parenteral agent, such as ceftriaxone, if community prevalence of fluoroquinolone resistance >10%.
**Consider a single dose of long-acting parenteral agent, such as ceftriaxone, if using TMP-SMX.
Alternative Therapies#:
Cefpodoxime 200 mg PO BID
Cefdinir 300 mg PO BID
#Beta-lactams are not preferred agents due to higher failure rates when compared to fluoroquinolones. Consider a single dose of long-acting parenteral agent, such as ceftriaxone, if using beta-lactams.
Duration of Therapy: 10-14 days
Take Home Point:
Utilize ciprofloxacin, levofloxacin, or TMP-SMX over beta-lactams when discharging patients with oral antibiotics for pyelonephritis.
Show References
Improving Compliance with Lung-Protective Ventilation
- Approximately 250,000 ED patients are intubated and receive mechanical ventilation each year in the United States.
- While emergency physicians understand the importance of providing lung-protective ventilation, current studies demonstrate that more than 40% of ED patients are placed on initial tidal volumes > 8 ml/kg of predicted body weight (PBW).
- In many cases, this may be due to the inaccurate estimation of patient height when determining PBW.
- In a recent single-center study, Tallman and colleagues evaluated a quality improvement intiative, whereby respiratory therapists were provided with a tape measure and an EHR BPA that reminded them to measure the patient's height for PBW.
- In this study, these simple, low-cost interventions significantly increased compliance with lung-protective ventilation.
- Take Home Pearl: Be sure to measure your intubated patient to accurately determine PBW and set the correct tidal volume.