Search
Acute lower back pain is a very common emergency department presenting complaint. Over the last several years there has been impetus to move away from opioids in the management of lower back pain.
A recent systematic review investigated the pharmacologic management of acute low back pain. This review looked at RCTs investigating the efficacy of muscle relaxants, NSAIDs, and acetaminophen for the treatment of acute nonspecific lower back pain of fewer than 12 weeks duration in patients > 18 years of age. Studies that investigated the use of opioids were not considered.
18 RCTs, totaling 3478 patients were included. 54% were women. The mean patient age was 42.5 ± 7.3 years. The mean length of follow-up was 8.0 ± 5.6 days. The mean duration of symptoms before treatment was 15.1 ± 10.3 days.
Results: Muscle relaxants and NSAIDs were effective in reducing pain and disability in acute LBP at approximately 1 week.
The combination of NSAIDs and acetaminophen was associated with a greater improvement than the sole administration of NSAIDs.
However, acetaminophen alone did not promote any significant improvement. Placebo administration was not effective.
Limitations: Most patients with acute LBP experience spontaneous recovery or at least reduction of symptoms, therefore, the real impact of most medications is uncertain. The present study wasn't able to distinguish among different classes of NSAIDs. A best practice treatment protocol cannot be extrapolated from this study.
Take home: In my practice, patients are treated with NSAIDs and Acetaminophen first line. I also include Licocaine patches for all patients. If there is a contraindication to NSAIDs, I treat with muscle relaxants alone.
This study highlights the lack of benefit of acetaminophen as mono therapy (which has been noted in other studies).
Show References
Background: Intranasal dexmedetomidine has seen usage in the anesthesia and sedation realms over the past few years, with an increasing interest in usage in the ED setting given its generally favorable safety profile and ease of administration. There has been specific interest and consideration in children with autism and neurodevelopmental disorders.
Study: Single center prospective provider study (compared to a retrospective group of patients under 18 who received oral midazolam for indications of agitation or anxiety via chart review) looking at patients 6 months to 18 years of age with an order for intranasal dexmedetomidine. Following use, a provider survey was completed to evaluate indication/rationale for use, satisfaction, comfort with use, and perceived time to onset as well as duration of effect.
Results: 29% of patients receiving IN dexmedetomidine experienced treatment failure compared with 20.7% of patients receiving oral midazolam (not statistically significant). In subgroup analysis, rates of treatment failure were lower for patients diagnosed with autism spectrum disorder receiving IN dexmedetomidine versus oral versed (21.2% versus 66.7%). Length of stay was longer in the IN dexmedetomidine group (6.0 hours versus 4.4 hours). Indication for use had variability between the two groups.
Bottom Line: IN dexmedetomidine may be a reasonable agent to utilize for anxiolysis in pediatric patients, especially those who have previously had paradoxical reactions or poor efficacy of benzodiazepines. It may be specifically useful when effects are desired for a slightly longer time and for non-painful/minimally painful interventions.
Show References
Background: The use of steroids in pneumonia has long been controversial with conflicting data, and the recent ESCAPe randomized controlled trial by Meduri et al. showing no mortality benefit with their use, but likely underpowered due to recruitment issues. The recently published CAPE COD study by Dequin et al. may change the game.
Design: Double-blind, placebo-controlled, multicenter, RCT
- 31 hospitals in France, 2015 to March 2020
- Adults with severe (P:F <300 on 50% FiO2 or NRB, mechanical ventilation, or pulmonary severity index >130) CAP (+symptoms and imaging)
- Notable exclusion criteria: vasopressors, aspiration-related, influenza, chronic steroids (equiv to >15mg prednisolone)
Intervention: Early hydrocortisone within 24 hrs, 200mg/day x 4-8 days depending on improvement, then preset taper
- 800 patients: 401 hydrocortisone, 399 placebo
Primary outcome: Death at 28 days
- Hydrocortisone 6% vs Placebo 12% (p = 0.006)
Secondary outcomes:
- Death at 90 days: Hydrocortisone 9.3% vs placebo 14.7%
- Decreased cumulative incidence of endotracheal intubation by day 28 (if not initially intubated)
- Decreased cumulative incidence of vasopressor initiation by day 28
- Higher median daily dose insulin in hydrocortisone group
- No difference in rate of hospital acquired infections or GIB
Bottom Line: The addition of hydrocortisone to antibiotics in severe CAP may decrease need for intubation and development of shock, and in this well-done study, decreased 28 and 90-day mortality.
Show References
A retrospective review of patients over age 13 presenting to one urban level one trauma center and one urban community hospital looked at traumatic injuries in patients presenting for sexual assault. They looked at 157 patients and found 61% of assailants were acquaintances, 22% strangers, and 15% intimate partners. One third of all patients had some traumatic injury however only 12 patients has serious injuries such as non-fatal strangulation or a fracture. Assault by an intimate partner was more likely to lead to injury/trauma including non-fatal strangulation. Drug and alcohol use was not associated with presence of injury.
Show References
Myasthenia gravis is an autoimmune disease of the neuromuscular junction, most commonly due to antibodies attacking acetylcholine receptors in the postsynaptic membrane. Up to 30% of patients with myasthenia gravis will experience a myasthenic crisis during their disease course. If rapid sequence intubation is indicated, the unique characteristics of this patient population must be considered in the event use of a paralytic is necessary. All paralytic agents can be expected to last significantly longer, and an unpredictable response may be seen with depolarizing agents - therefore non-depolarizing agents are preferred in this population.
Non-Depolarizing Agents (Rocuronium, Vecuronium)
- MG patients have increased sensitivity to non-depolarizing agents and require lower doses than typically used
- It is reasonable to dose non-depolarizing agents at one-half the standard dose used. For example, rocuronium would be dosed at 0.5-0.6 mg/kg instead of the standard 1-1.2 mg/kg
Depolarizing Agents (Succinylcholine)
- MG patients have decreased expression of normal acetylcholine receptors which are required for depolarizing agents to work effectively and require higher doses than typically used
- Succinylcholine is typically dosed at 1.5-2.0 mg/kg (roughly double the dose used in other patient populations)
Show References
The classic teaching is that patients with acute pancreatitis should be aggressively hydrated with IV fluids. But as we increasingly question heavy handed fluid strategies in other areas such as sepsis, should we look at pancreatitis management too?
Li et al did a systematic review of the literature on aggressive fluid resuscitation (the exact protocol/definition varied per study, but we're mostly talking 15-20 mL/kg boluses followed by 3-5 mL/kg/hr infusion) vs less aggressive fluid resuscitation (mostly 10 mL/kg boluses followed by 1.5 mL/kg/hr infusion). They found that aggressive resuscitation worsened mortality in severe pancreatitis (RR 2.45) and trended towards worse mortality in non-severe pancreatitis (RR 2.26, but CI crossed 1). Aggressive was associated with more complications in both severe and non-severe pancreatitis pancreatitis.
Multiple society guidelines still call for aggressive IVF resuscitation for acute pancreatitis, but probably need to be updated given mounting evidence that this is harmful. More recent guidelines suggest "goal-directed therapy", but no one is completely sure what that means.
Bottom Line: In acute pancreatitis, a more conservative empiric IVF resuscitation is probably better than the clasically taught aggressive approach. Whether even less fluids would be better or worse is not known, but for now it's probably best to stick to a 10 mL/kg bolus and 1-2 mL/kg/hr infusion when ordering fluids for these patients unless you have another indication.
Show References
This study is a secondary analysis of another studying looking at hypertonic saline in traumatic brain injury (TBI) making it not the most robust study however it found that TBI patients who’s PaO2 dropped below 100 had a worse outcome than those whose PaO2 did not fall below 100.
Bottom line: This is a reminder that traumatic brain injury patients do not do well with hypoxia or hypotension even if transient (during intubation, etc.). Pre-oxygenate and resuscitate prior to intubation and maintain oxygen saturations in the mid-90s for your traumatic brain injured patients. This applies to prehospital, emergency department, and ICU settings
Show References
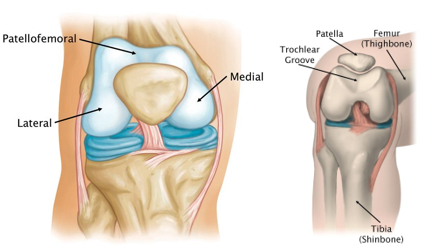
Patellofemoral anatomy and disease (part 1)
During normal knee flexion, the patella slides within the trochlear grove. Both (patella and the trochlear groove) are lined with articular cartilage at the patellofemoral articulation.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint2.jpg
{kind=link}
Multiple forces act on the patella which can affect proper tracking: Proximately, by the quadriceps tendon, distally, by the patellar tendon, medially, by the medial retinaculum/vastus medialis and laterally by the lateral retinaculum and the vastus lateralis.
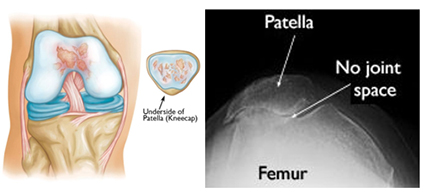
Patellofemoral OA can occur when this cartilage starts to wear and can be seen in skyline/sunrise/notch or equivalent views. OA here rarely occurs in isolation (<10%) and is usually part of medial or lateral knee OA.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint3.jpg
{kind=link}
Patellofemoral pain is usually from overuse/training overload or malalignment.
Contributors to overuse involve total joint load which may have influence from training volume (total miles), intensity (competitive sports) in addition to BMI (>25) in addition to overall fitness level.
Malalignment aka abnormal patellar tracking involves both static (leg length discrepancy, hamstring tightness, etc.) and dynamic components (hip weakness, gluteus medius weakness, excessive foot pronation, etc.).
Patients with anterior knee pain should have activity modification, ice, NSAIDs (not steroids) and long-term engagement in physical therapy (>6 months) with a focus on flexibility and strengthening of lower extremity kinetic chain including the vastus medialis, gluteus medius, hip external rotators and core.
Also, consider looking for hyper supination or pronation. Foot orthotics can be of help with this.
Things to Consider for Persistent or Worsening Septic Shock
- Septic shock is one of the most common critical illnesses in emergency medicine and critical care.
- Norepinephrine is recommended as the initial vasopressor of choice for patients with septic shock, with vasopressin or epinephrine commonly added as a second vasopressor for patients with refractory shock.
- While vasopressors are being added and titrated, it is important to consider additional diagnoses in patients with worsening or persistent septic shock. Some of these diagnoses include:
- Undetected infection that requires emergent source control
- Concomitant causes of shock: cardiogenic, PE, abdominal compartment syndrome, tamponade, adrenal insufficiency
- Severe acidosis
- MAP underestimation by a radial arterial line
Show References
Predicting the need for a mass hemorrhage protocol (MHP) activation is important both for individual patient outcome as well as for proper utilization of critical resources such as blood products and healthcare workers time and effort. These two studies look at using the RABT score to predict the need for mass transfusion. The RABT score is:
A 4-point score
blunt (0)/penetrating trauma (1),
shock index (hr/SBP)≥ 1 (1),
pelvic fracture (1)
FAST positive (1)
With a score >2 predictive of needing MHP.
These studies (one in Canadian trauma centers, the other in US trauma centers) validate the use of this score to predict the need for activation of a mass hemorrhage protocol.
Show References
Show References
This study from Sweden looked at 2397 trauma patients and identified 768 with thoracic injury. Those with thoracic injury had a 30-day mortality of 11% whereas those without thoracic injury had a 4% 30-day mortality. Patients over age 60 had higher mortality and were more likely to have rib fractures. Those under 60 with thoracic injury were more likely to have thoracic organ injury than rib fracture.
Bottom line: Rib fractures were more common over age 60 and there was a higher mortality for those with thoracic vs non-thoracic trauma.
Show References
Title: Electrocardiographic Changes at the Early Stage of Status Epilepticus: First Insights From the ICTAL Registry.
As the song goes: “the thigh bone is connected to the hip bone, the hip bone is connected to the back bone.” It turns out that the brain electrical activities are also connected to the heart conduction activities.
In a multi-center (23 French ICUs) retrospective analysis of 155 critically ill patients with status epilepticus, ECGs were done within 24 hours of onset of status epilepticus, and were independently reviewed by cardiologists showed abnormalities in 145 (93.5%) of patients.
Below is a list of events that occurred more than 10% of events.
Abnormal rate (<60 or > 100 beats/min 64 (44%)
Negative T-waves 61 (42%)
Flattened T-waves 18 (12%)
ST elevation 24 (16.6%)
ST depression 26 (17.9%)
Left axis deviation 22 (15.9%)
Discussion:
Major ECG abnormalities were not associated with 90-day functional outcome in multivariable logistic regression.
The brain-heart axis could be affected by antiseizure medication. For example, phenytoin, lacosamide are sodium channel blockers while benzodiazepines, propofol, barbiturates with their GABAnergic effects will also display cardiac side effects. This current study was not able to tease out whether the cardiac effects were from medication. Therefore, further studies are needed to figure out the cardiac effect for patients with status epilepticus.
Show References
Applying a cervical collar to all patients involved in motor vehicle collisions and mechanical falls has been shown to add to patient discomfort, unwarranted imaging studies and prolonged on scene time for emergency medical services. This study adds further evidence that paramedics can use validated algorithms to clinically clear cervical spine injuries without any bad outcomes including spinal cord injuries. EMS medical directors and all of us who interact with EMS providers should be proactive in developing protocols to use cervical immobilization in appropriately selected patients only. This study used the Modified Canadian C-Spine Rule.
Show References
Non-dihydropyridine calcium channel blockers, verapamil and diltiazem, can induce hypotension when administered intravenously (IV) in approximately 4% of patients. It has previously been taught that administering IV calcium before administering these medications may prevent the hypotension. Previously, this theory was tested for verapamil and found success with reducing hypotension. Only one study has been done exclusively with diltiazem and it found no benefit.
In a new multicenter retrospective cohort study of adults in the ED, patients were randomized into two groups: those who received diltiazem alone and those who received calcium with diltiazem for atrial fibrillation/atrial flutter (AF/AFL) with a HR ≥ 120 bpm. Patients were excluded if they required electrocardioversion, had other agents prior to diltiazem, incomplete information, were pregnant or incarcerated. The primary outcome was change in SBP 60 minutes (+/-30 minutes) after diltiazem administration.
Baseline characteristics: 73 year old, equal male:female, predominantly white patients. 40% had new onset AF/AFL and the initial HR was 140 in both groups. There were 198 patients in the diltiazem group and 56 patients in the combination group. Notably, patients in the combination group had a lower presenting SBP 109 (101-121) vs 123 (114-132) P<0.0001 which matches classical teaching for when to consider calcium use. Additionally, patients in the combination group received a lower diltiazem dose of 10mg vs 15mg in the monotherapy group p=0.004 with both group receiving doses lower than the standard 0.25 mg/kg dosing recommendation.
Outcomes:
- Median change in SBP was not different between the monotherapy and combination therapy groups: (-2 mmHg vs -1.5 mmHg, p= 0.642)
- There was no difference in:
- Time to rate control (1.4 vs 1.8 hours, p= 0.141)
- Time to sustained rate control (7.9 vs 7.7 hours, p=0.570)
- Change in HR at 60 minutes: (-33 vs -34 bpm, p=0.428)
- A subgroup analysis looking at timing of calcium (i.e. before or with diltiazem administration) also found no difference.
Take Home Point:
Administration of IV calcium may not be as beneficial as previously thought to prevent hypotension induced by diltiazem administration. This particular study is confounded by the relatively low doses of diltiazem overall, but utilizing a lower dosing strategy in patients with low SBP is a reasonable safety strategy.
Show References
Background:
There have been a few studies that suggested that there may be some neuroprotective effect with a higher MAP goal in post-arrest patients. However, these studies were small and/or observational.
Intervention:
-The BOX trial was a double-blind, dual-center (Denmark), randomized trial
-Study population: >18 yo, OHCA of presumed cardiac cause
-Pts randomized to higher (77 mmHg) vs. lower (63 mmHg) MAP goal
-double-blinded by attaching a module that reported a BP that was 10% higher or lower than the pt’s actual BP
-Notable exclusion criteria:
-unwitnessed asystole or suspected intracranial bleeding/stroke
Results/Primary outcome:
-No sig difference in composite of death + Cerebral Performance Category of 3 or 4 (3= severe disability, 4= coma) within 90 days
-133 patients (34%) in the high-target group vs 127 patients (32%) in the low-target group (hazard ratio, 1.08;95%CI, 0.84 to 1.37; P=0.56)
Caveats/Takeaways:
-Mean difference in BP was 10.7 mmHg (95[CI], 10.0 to 11.4) which is still relatively clinically significant, but was lower than their goal difference of 14 mmHg
-They used IVF to target a CVP of 10 mmHg prior to initiation of norepi and used dopamine "if necessary"
-Consider generalizability given study population was patients with presumed cardiac cause of arrest
-Keeping a lower MAP goal of >65 mmHg is reasonable in post-arrest patients
Show References
In a small study at a single level one trauma center, ? of patients screened positive for illicit fentanyl use prior to violent or intentional injury. Those who screened positive were more likely to require ICU admission and had a higher rate of previous trauma center admission. The authors concluded:
“Exposure to illicit fentanyl was common among victims of violence in this single-center study. These patients are at increased risk of being admitted to intensive care units and repeated trauma center visits, suggesting fentanyl testing may help identify those who could benefit from violence prevention and substance abuse treatment.”
Show References
Question
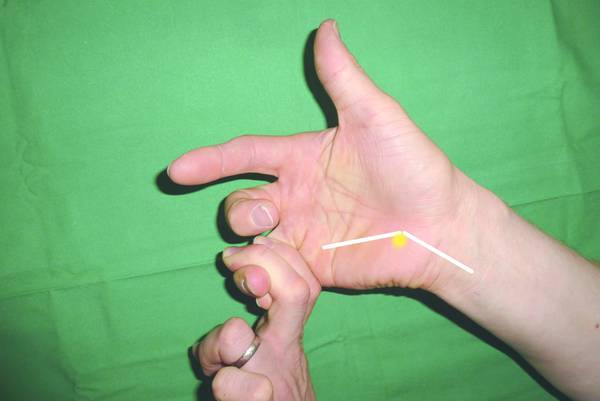
21-year-old college softball player presents for evaluation of Left hand/wrist pain following batting practice.
She states her pinky is “tingly”
On exam, there is tenderness over her volar ulnar wrist.
You obtain an X-ray.
https://prod-images-static.radiopaedia.org/images/52314027/a662d8f338ec08ba56178463638d25_jumbo.jpeg
{kind=link}
What’s the diagnosis?
Show Answer
{kind=link}
{kind=link}
Given my previous post on APRV (11/6/2022) and while I take issue with many of the author's statements, I wanted to share a very well referenced article with an excellent discussion on the current gaps in the knowledge around APRV and its use.
One statement I do agree with is the need for a well-designed and adequately powered trial of this mode in an admittedly difficult-to-study population.
Fortunately, this article has an invited rebuttal pending from Dr. Habashi which I am sure will appear in the Educational Pearls in short order.
Good luck to the residents on the ITE!
Show References
This study looked at 69,321 head injured patients over age 65 in a health care database for delayed intracranial hemorrhage (within 90 days of visit). 58,233 patients were not on oral anticoagulants, 3081 (4.4%) were on warfarin and 8007 (11.6%) were on direct oral anticoagulants. One percent of patients not on anticoagulation and those on oral direct anticoagulation had a delayed hemorrhage while those on warfarin had a 1.8% delayed hemorrhage rate.
Bottom Line: Direct oral anticoagulants do not increase the risk of delayed intracranial hemorrhage in patients over age 65 from baseline but warfarin does.