Search
- A recent meta–analysis of 12 studies (6,538 patients with 1,824 ROSC) assessed the quality of cardiopulmonary resuscitation (CPR) using either manual vs. mechanical (load-distributing or piston-driven) compressions in out-of-hospital cardiac arrest
- Compared w/manual CPR, load-distributing band CPR had significantly greater odds of ROSC (odds ratio, 1.62 and p<0.001)
- The treatment effect for piston-driven CPR was similar to manual CPR
- The difference in percentages of ROSC rates from CPR was 8.3% for load-distributing band CPR and 5.2% for piston-driven CPR
- Compared with manual CPR, combining both mechanical CPR devices produced a significant treatment effect in favor of higher odds of ROSC with mechanical CPR devices (odds ratio, 1.53 and p<0.001)
Show References
Treatment of Severe Hypothyroidism
We do not see patient's with severe hypothyroidism often, but it is important that they be treated aggressively. Some treatment pearls are
- Rule out aggravating cause (i.e.: infection [UTI, pneumonia], myocardial infarction)
- Start IV levothyroxine dosing
- Initial dose 400-500 mcg. This is a large dose but it only saturates the thyroid receptors and will not cause a rebound hyperthyroidism state.
- Daily dose 100 mcg/day
- Consider starting Dexamethasone/hydrocortisone
- Patients may also have adrenal insufficiency from primary pituitary failure or may have secondary adrenal suppression due to the severe hypothyroidism. If dexamethasone/hydrocortisone is not provided they may develop severe adrenal insufficiency once you kick start their metabolism.
Lactate is commonly used in the adult ED when evaluating septic patients, but there is a lack of literature validating its use in the pediatric ED. Pediatric studies have suggested that in the ICU population, elevated lactate is a predictor of mortality and may be the earliest marker of death.
A retrospective chart review over a 1 year period showed that one elevated serum lactate correlated with increased pulse, respiratory rate, white blood cell count and platelets. Serum lactate had a negative correlation with BUN, serum bicarbinate and age. Elevated lactate levels were higher for admitted patients. However, the mean serum lacate level was not statistically different between those diagnosed with sepsis and those that were not.
The study included 289 patients less then 18 years who had both blood cultures and lactate drawn. This community hospital had a sepsis protocol in place that automatically ordered a lactate with blood cultures. Only previously healthy children were included.
The study is limited by its small sample size and overall low lactate levels. Despite having a protocol in place, only 39% of patients who had blood cultures drawn had lactate levels available for analysis. The mean serum lacate in this study was 2.04 mM indicating that the study population may not have been sick enough to determine mortality implications. There were no serial measurements.
Bottom line: Consider measuring serum lacate in your pediatric patient with suspected sepsis. Pediatric ICU literature does suggest that an serum lactate as low as 3mM is associated with an increased mortality in the ICU.
Show References
The internet has become a wealth of information and some books have now gained internet noteriety. A chemist and author of the book - TIKHAL: Tryptamines I Have Known and Loved is an excellent example.
Tryptamines include drugs like LSD and alpha-methyltryptamine (AMT). Vivid visual hallucinations and serotonin agonism, these drugs were glamorized by this author. He would synthesize a tryptamine and then "taste it". Take a look at the link below where he first describes the biochemical synthesis he performed then describes his dose response effect when he tried the drug.
If you run into a drug or slang term in the ED you are not familiar with, the website www.erowid.org will likely have the translation.
http://www.erowid.org/library/books_online/tihkal/tihkal48.shtml
COPD treatment guidelines (e.g., GOLD) recommend 10-14 days of steroid therapy following a COPD exacerbation to prevent recurrences; the supporting data is weak.
A recent noninferiority trial (here) compared patients with a severe COPD exacerbation who received either a 5-day course (n=156) or 14-day course (n=155) of prednisone 40mg.
The results were:
- No significant reduction in time until the next exacerbation (primary end-point)
- No significant difference in mortality, incidence of mechanical ventilation, FEV1, or dyspnea scores (secondary end-points)
What you need to know:
- This was a non-inferiority trial, which has limitations
- All subjects received broad-spectrum antibiotics and an initial dose of IV steroid
- Surprisingly, there were no differences between groups with respect to steroid complications (e.g., hyperglycemia, hypertension, etc.)
Bottom-line: 5 days of prednisone may be as effective as 14-days for COPD exacerbations.
Show References
Question
46 year-old female presents with a headache. The following is seen on visual inspection of the eye. What's the diagnosis?
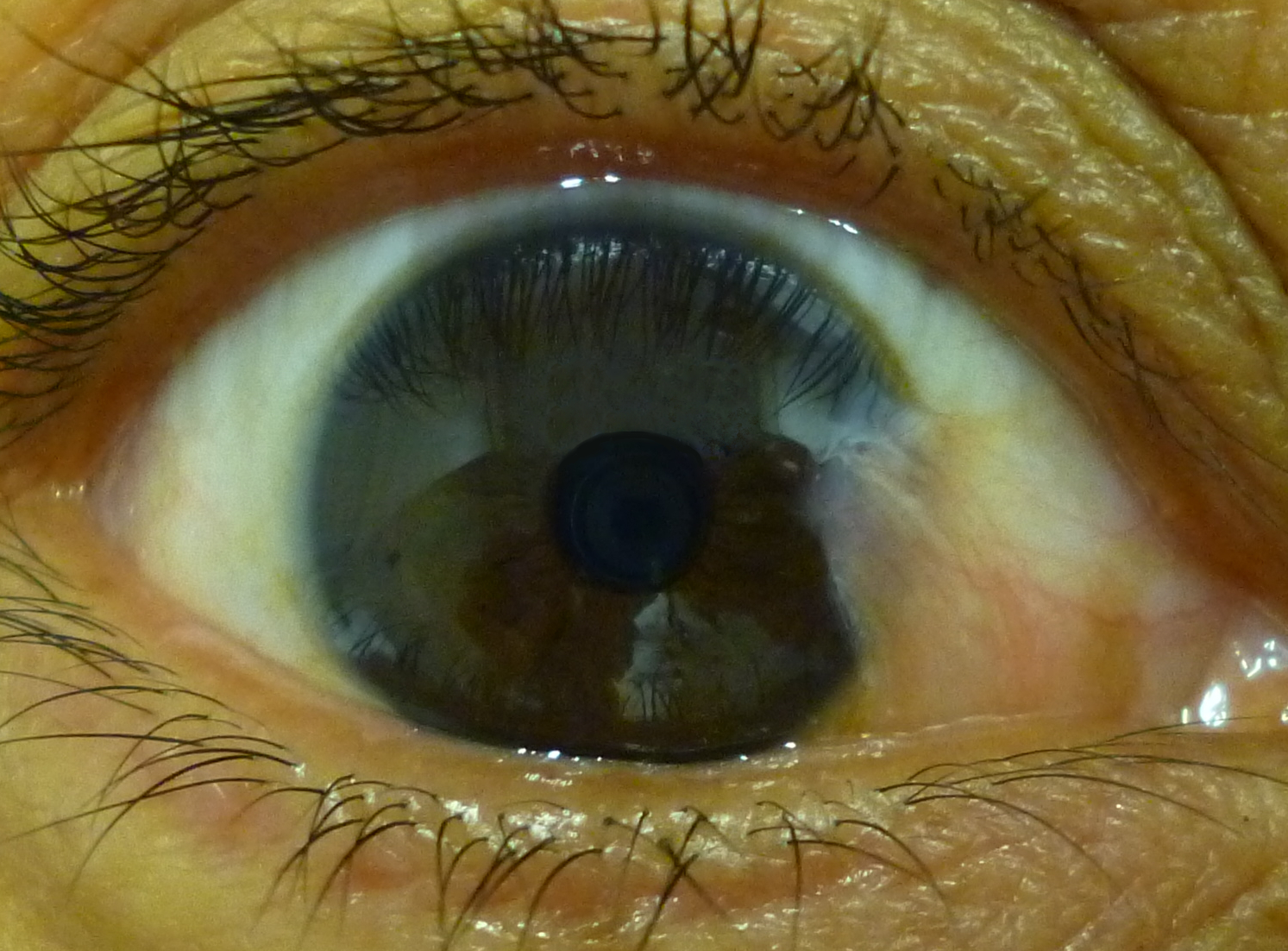
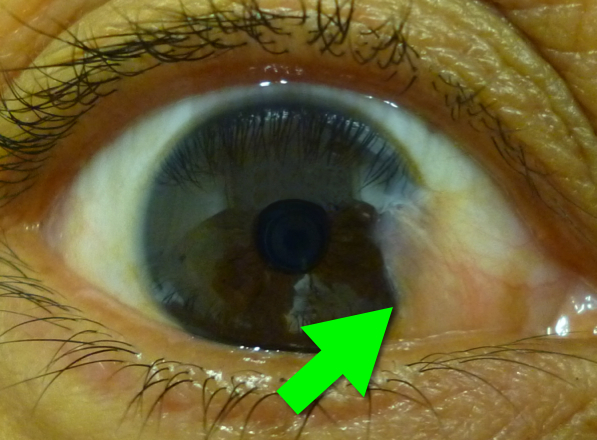
Show Answer
{kind=link}
Show References
Radiation therapy is frequently utilized in the management of numerous thoracic malignancies
Cardiovascular disease is now the leading cause of nonmalignancy death in radiation-treated cancer survivors
The spectrum of radiation-induced cardiac disease is broad
The relative risk of CAD, CHF, pericardial/valvular disease, and conduction abnormalities is particularly increased
Early identification of potential cardiac complications w/cardiac MR and echocardiography provides an opportunity for regular assessment and potentially improved long term mortality
Show References
Tests for distal ulnar nerve entrapment
Ask patient to hold a piece of paper between the thumb and the index finger
Normally this is a fairly simple task.
With an unlar nerve palsy, the patient will substitute with the FPL (flexor pollicis longus - median nerve innervation). This causes flexion of the thumb in order to maintain the grip since the adductor pollicis cannot be used. This causes thumb flexion rather than extension.
http://www.mims.com/resources/drugs/common/CP0042.gif
http://www.youtube.com/watch?v=yJTIhm1VfSI
Risk stratisfication score introducted by Maden Samuel in 2002.
The Pediatric Appendicitis Score had a sensitivity of 1, speciificity of 0.92, positive predictive value of 0.96, and negative predictive value of 0.99
Signs:
- Right lower quadrant tenderness = 2 points
- Cough/Percussion/Hop RLQ tenderness = 1 point
- Pyrexia = 1 point
Symptoms:
- RLQ migration of pain = 1 point
- Anorexia = 1 point
- Nausea/Vomiting = 1 point
Laboratory Values:
- Leukocytosis = 2 points
- Polymorphonuclear neutrophiia = 1 point
Scores of 4 or less are least likely to have acute appendicitis, while scores of 8 or more are most likely.
Show References
In June 2013 the American College of Medical Toxicology (ACMT) released a Guidance Document on the Management Priorities in Salicylate Toxicity. Here are some key highlights:
- Continuous IV infusion of sodium bicarbonate is indicated even in the presence of mild alkalemia from the early respiratory alkalosis.
- Euvolemia is important.
- If intubation is required, administration of sodium bicarbonate by IV bolus at the time of intubation in a sufficient quantity to maintain a blood pH of 7.45-7.5 over the next 30 minutes is a reasonable management option during this critical juncture.
- Once airway control has been established, it is imperative that the increased minute ventilation and low PCO2 usually seen with salicylate intoxication are maintained.
- A salicylate concentration approaching 100 mg/dL warrants consideration of hemodialysis in the acute toxicity setting (40 mg/dL for chronic toxicity). Consult nephrology well before these threshold levels.
The full document can be accessed here.
The Poison Review blog by Dr. Leon Gussow discusses the guidance document here.
Follow me on Twitter (@PharmERToxGuy)
Question
3 year-old male develops rash 5 days after starting amoxicillin for acute otitis media. What's the diagnosis?

Show Answer
Show References
- Typically the normal ECG shows progression of T-wave size across the precordial leads & the T-wave in V1 is inverted or flat
- A large upright T-wave in V1 can be considered normal when there is high voltage/LVH or LBBB
- A new upright T-wave in V1 can be indicative of significant atherosclerotic disease
- If the T-wave in V1 is larger than the T-wave in V6 have a high suspicion for myocardial disease
- A new tall upright T-wave in V1 has ~84% specificity for ischemic heart disease (Barthwal)
Show References
A recent, randomized study evaluated two approaches for treating acute pain in an inner-city ED.
- Group 1 received hydromorphone 2 mg. Group 2 received hydromorphone 1 mg (with the option of a second 1 mg dose 15 minutes later).
- 1 hour after the dose, patients were asked if they wanted more pain medication.
- Both groups had an equal proportion of patients decline more pain medication at one hour (67%). 61% of patients in the 1 + 1 group only needed the initial dose of hydromorphone!
- Secondary outcomes and safety measures were also similar between the groups.
- Patients with chronic pain, age >64, weight <150 pounds, or opioid use within last 7 days were excluded.
Application to clinical practice: For most patients with acute, severe pain in the ED, start with hydromorphone 1 mg. It may be all the patient needs and can potentially avoid giving them extra opioid they don't need.
Show References
- Hold metformin if the patient is at risk for dehydration (eg. vomiting, diarrhea) due to the risk of lactic acidosis
- Medications that stimulate insulin secretion (eg. sulfonylureas, repaglinide, or nateglinide) should be held if the patient is at risk for hypoglycemia
- Patients usually should continue their basal insulin, but may decrease or hold their bolus dosing.
- Finger sticks should be checked every 2-4 hours for those on insulin, or 2-4 times per day for type II diabetics not on insulin.
Show References
Background:
Infection with the Hepatitis C virus can result in mild to severe liver disease. Morbidity and mortality from Hep C is increasing the US--many of the 2.7-3.9 million persons with Hep C are not aware of their infection.
Pertinent Information:
- Hepatitis C is now curable for many patients
- Current treatment recommendations are a combination of medications (pegylated interferon plus ribavirin plus a protease inhibitor).
- Research in this field is very active--treatment is likely to change in the next 3-5 years.
- Risk reduction strategies to protect the liver (i.e. eliminating alcohol and Hep A and B vaccination) are also recommended.
Critical New Recommendation
As much of the disease burden is in the “Baby Boomers,” the CDC now recommends one time testing of all persons born between 1945 and 1965.
Bottom Line:
While emergency department management is focused on the treatment of acute complications of liver disease, it is also important to have all age appropriate patients follow-up for testing and treatment of Hepatitis C with their primary care provider.
Show References
Hydroxyethyl starch (HES) is a colloid used for volume resuscitation in critically-ill patients.
Previous studies (click here) have compared crystalloids to HES during fluid resuscitation and have demonstrated that HES has an increased cost with more adverse effects. Adverse effects may include:
- Coagulopathy
- Acute kidney injury
- Increased mortality
In the United States, the Federal Drug Administration published a warning on June 24th 2013 with respect to the use of HES in critically ill adult patients. Specifically, it warned about the use of HES in patients,
- with sepsis
- with pre-existing kidney injury
- admitted to the ICU
- undergoing heart surgery with cardiopulmonary bypass
If a decision to use HES is made, the FDA warning advises to:
- discontinue use of HES at the first sign of renal injury or coagulopathy
- continue to monitor renal function for at least 90 days (all patients)
Bottom line: With an increased cost and evidence of harm compared to crystalloids, it appears the indications for use of HES are rapidly declining.
Show References
Question
65 year-old male presents with nausea and diffuse abdominal pain, 3 days after knee replacement surgery. What's the diagnosis?
Show Answer
Show References
- Statin therapy significantly reduces the risk for thrombotic events
- A recent study sought to determine the impact of short-term intensive statin therapy on intracoronary plaque lipid content
- 87 patients with multivessel CAD undergoing percutaneous coronary intervention and at least 1 other severely obstructive were randomized to intensive (rosuvastatin40 mg daily) or standard-of-care lipid-lowering therapy
- Upon follow-up, median reduction (95% confidence interval) was significantly greater in the intensive versus standard group ( p=0.01)
- Short-term intensive statin therapy in small trials reduces lipid content in obstructive lesions and further large studies with longer follow-up are warranted
Show References
Sternal fractures
- Initially thought to be associated with high mortality due to associated injuries though newer studies show the mortality rate is about 1%.
- Can be associated with
- Rib fractures
- Mediastinal injury
- Cardiac Contusion
- Pneumothorax
- Aortic dissection
- Pulmonary Contusion
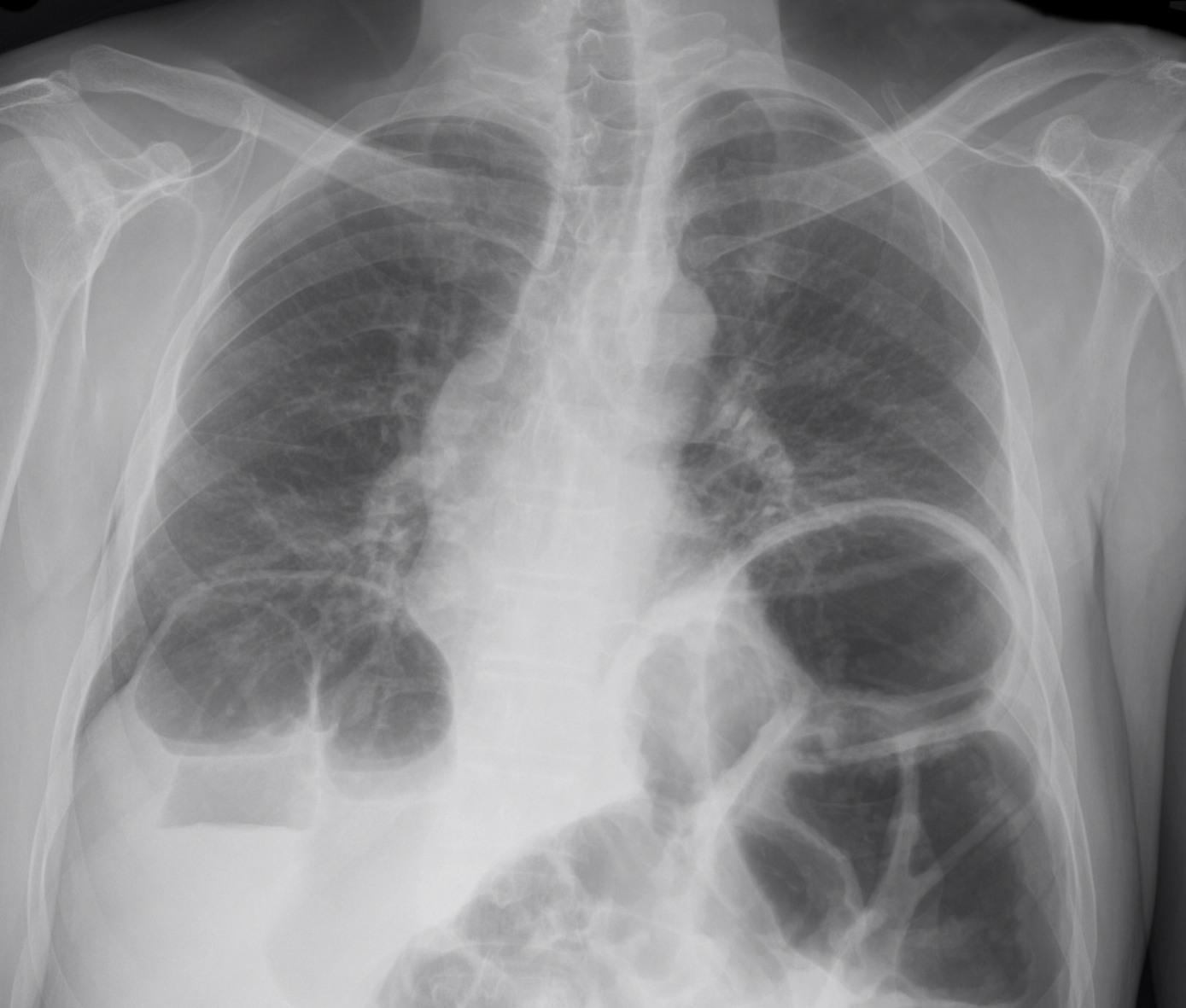
- The diagnosis can be made with plain radiographs, but a fracture can be missed on a regular PA and Lateral Chest Xray. Ask for dedicated sternal views to better define the fracture
- CT Chest is only needed if you are concerned about associated injuries
- Obtain an ECG on arrival and at 6 hours to ensure there are no signs of a myocardial contusion
- ST segment changes, arrhthymias
- Treatment is supportive. Provide adequate pain control and treat associated injuries
Show References