Search
General Information:
Ebola is a deadly hemorrhagic fever of the virus family Filoviridae.
- The largest outbreak known is currently affecting multiple countries in West Africa (especially Guinea, Liberia and Sierra Leone).
- As of July 23rd, the WHO has recorded a total of 1,201 cases and 672 deaths (case fatality rate of 56%).
Clinical Information:
- Spread by close contact (direct contact with body fluids)
- Primarily seen in family members of those infected and health care workers
- Incubation is usually from 8-10 days (can be from 2-21 days)
- Typical signs and symptoms include: fever, headaches, muscle/joint aches, abdominal pain, vomiting, diarrhea
- Additionally, some patients may experience: rash, red eyes, chest pain, difficulty breathing, difficulty swallowing, bleeding from multiple areas
Treatment and Public Health
- Supportive care and treatment of complications
- Contact isolation
- Immediately report to the local health authorities
Bottom Line:
While the likelihood of general dissemination to the general U.S. population is very low, U.S. healthcare workers need to be aware and alert for the signs and symptoms of Ebola for patients recently returned from West Africa.
Show References
Observation after giving IM Epi for allergic reactions or anaphylaxis
Background
- Common practice is to observe patients who receive epinephrine for allergic reactions or anaphylaxis for several hours post-administration
- This can be from 4-24 hours depending on the institution
- This is to monitor for a biphasic reaction
Question
- Do we need to observe these patients?
- And if so, for how long?
Meta-analysis
- 2 urban Canadian EDs
- 5 year period
- Primary outcome was the amount of patients with a clinically important biphasic reaction
- Secondary outcome was mortality
Results
- 2819 encounters: 496 anaphylactic + 2323 allergic reactions
- 5 clinically important biphasic reactions (0.18%; 95% CI 0% to 0.17%)
- No fatalities
- Biphasic reactions tended to happen several hours (>24hrs) after ED discharge
Limitations
- If patients did not return to an ED in the region, then they would not be identified as a possible biphasic reaction
What to do?
- You can probably discharge most patients whose symptoms have resolved without a prolonged observation period (<4hrs)
- Patients with ongoing anaphylaxis and allergic reaction, should be observed longer or admitted
- Biphasic reactions are very rare
Show References
Question
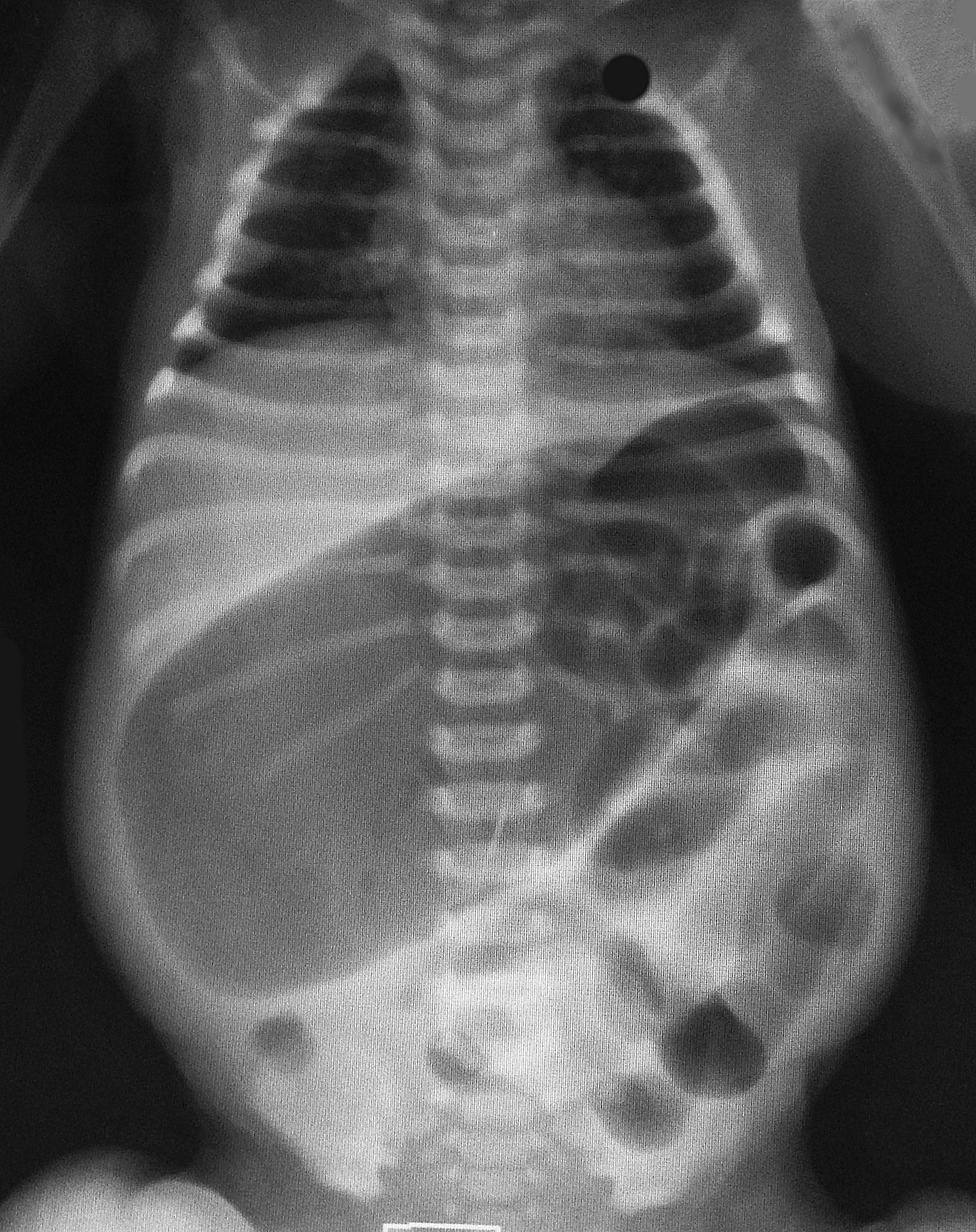
2-day old baby boy presents with forceful vomiting of entire feeds, bloated belly, and has not passed stools since birth. What's the diagnosis?
Show Answer
Show References
HIV & Atherosclerosis
Advances in antiretroviral treatment has increased the life expectancy of patients with HIV significantly, AIDS-related deaths have fallen by 30% since they peaked in 2005.
HIV infection predisposes to a chronic inflammatory and immunologic dysfunctional state, subsequent highly active antiretroviral treatment (HAART) results in metabolic changes and dyslipidemia.
In the post-HAART era, CAD is now considered to be the main cause of heart failure in HIV-infected patients, superseding the prior most common etiologies myocarditis and opportunistic infections.
The presentation of CAD in HIV-infected patients is largely similar to that in the general population with the exception is that they present at a younger age.
Certain antiretroviral agents specifically protease inhibitors have conventionally been associated with lipid dysfunction, further complicating the HIV-infected patients milieu.
Recent research has shown that a C-C chemokine receptor-type 5 (CCR5) antagonists has emerged as a potential target both as an antiretroviral agent as well as in the process of arresting atherogenesis, but warrants more research.
Show References
Cervical Cord Neuropraxia (CCN)
A concussion of the spinal cord as a result of an on-field collision.
A transient motor and/or sensory disturbance, lasting less than 24 hours.
A distinct and separate entity from spinal cord injury resulting in quadriplegia
Incidence 7.3 per 10,000 athletes
Approx. 50% of players experiencing CCN who return to play, have a second episode
The risk of this second episode is inversely proportional to the size of the cervical bony canal
Athletes with narrow canal diameter are more likely to have a 2nd episode
Those with normal canal diameter (14 mm on MRI) have a 5% risk
Those with a narrow canal (9 mm or less)) have a greater than 50% risk.
Whether repeat episodes lead to permanent spinal cord injury is unknown
Show References
Ondansetron is a highly effective anti-emetic that, since it has gone generic, is also quite inexpensive. There have been some reports of QT prolongation and cardiac arrhythmias especially with the high-dose 32mg IV dose for chemotherapy patients.
Is still safe in our ED population? A large systematic review was done in this month's Ann Emerg Med July 2014,p19-31.
Take Home Points:
1) No reports of arrhythmia associated with single dose administration identified
2) 80% of 60 unique reports were IV
3) 83% had significant PMH or already on a QT prolonging drug
Conclusion: Ondansetron doesn't warrant routine EKG or electrolyt screening in oral administration.High dose IV and High Risk patients do require more vigilance with EKG and electrolyte screening.
Maybe not! A new prospective study looked at 600 adult trauma patients presenting with mild traumatic intracranial hemorrhage (with a GCS 13-15), and derived a clinical instrument that predicted the need for a “critical care intervention” (and therefore needing an ICU level of care). These interventions included intubation, neurosurgical intervention and need for invasive monitoring, among other things.
The derived instrument consisted of 4 variables:
1. GCS less than 15
2. Non-isolated head injury
3. Age 65 years or older
4. Evidence of swelling or shift on the initial head CT
The presence of at least one of these variables predicted the need for critical intervention, identifying 114 of the 116 patients who actually did require it, making it 98.3% sensitive.
This clinical decision rule is yet to be externally validated.
Show References
Predicting Neurologic Outcome in Patients Treated with TTM
- Whether you target 36oC or 33oC, targeted temperature management (TTM) improves survival and long-term neurologic oucome in survivors of out-of-hospital cardiac arrest.
- TTM, however, can affect the accuracy and timing of commonly used tests to predict poor neurologic outcome.
- Golan, et al just published a meta-analysis evaluating the accuracy of select diagnostic tests to predict outcome in patients treated with TTM.
- 20 studies (1,845 patients)
- Most accurate tests to predict poor neurologic outcome were:
- Bilaterally absent pupillary reflex (LR 10.45)
- Bilaterally absent somatosensory-evoked potentials (LR 12.79)
- Specificity of tests improved when testing was delayed > 72 hours
- Other commonly used tests (i.e., corneal reflexes, GCS motor score, unfavorable EEG readings) had higher false positive rates and lower LRs
Show References
Question
45 year-old right-hand dominant patient presents with right hand pain from a prior injury to hand. Patient has also been injecting subcutaneous heroin into hand for relief. What's the diagnosis?

Show Answer
Show References
ECG Risk Predication in ARVD
Arrhythmogenic right ventricular dysplasia (ARVD) is a genetically determined cardiomyopathy characterized by fibrofatty replacement of the right ventricle (RV) predisposing to ventricular arrhythmias, heart failure, and sudden cardiac death (SCD).
Twelve-lead electrocardiography (ECG) is an easily obtainable and noninvasive risk stratification tool for major adverse cardiac event (MACE); defined as a composite of cardiac death, heart transplantation, survived sudden cardiac death, ventricular fibrillation, sustained ventricular tachycardia, or arrhythmic syncope.
ARVD ECG findings that predict adverse outcome are not well known.
A multicenter, observational, long-term study, found ECG findings were quite useful for risk stratification of MACE, specifically:
- Repolarization criteria
- Inferior leads T wave inversions
- Precordial QRS amplitude ratio of ≤0.48
- QRS fragmentation
Show References
· Smallpox (Variola):
o Only eradicated human infectious disease.
o Prior to the advent of vaccination, it killed an estimated 400,000 Europeans annually and was a major cause of blindness.
· Major potential as a bioterrorism agent:
o Now only supposed to exist in two laboratories in the world (at the CDC in Atlanta, Georgia and in the Vector Institute in Koltsovo, Russia).
· Recently, previously unknown vials of active virus from the 1950s were found in a NIH laboratory in Maryland.
· Clinical Presentation:
o Incubation is usually 10-12 days (range 7-17 days)
o Signs and symptoms include:
§ Febrile (38.8-40.0C) prodome lasting 1-4 days, headache, myalgia (esp. back/spinal pain), pharyngitis, chills, abdominal pain
§ Rash: classically round and well circumscribed. May be confluent or umbilicated. The rash evolves slowly: macules to papules to pustules to scabs.
· It is important to differentiate smallpox from chicken pox (Varicella):
o Smallpox: Significant prodrome. Centrifugal rash (trunk to extremities). Can involve soles and palms. Lesions are in the same stage of development on any one part of the body.
o Chickenpox: Minimal prodrome. Centripetal rash (extremities to trunk). Seldom on soles and palms. Asynchronus evolution of rash.
Bottom Line:
Smallpox is a global public health emergency and requires immediate reporting. If the clinical presentation is unclear, discuss with local infectious disease experts or public health officials.
Show References
Up to 26% of patients with tympanostomy tubes (PE tubes) can suffer from clinically manifested otorrhea. This is thought to be the result of acute otitis media that is draining through the tube. Previous small studies suggested that antibiotic ear drops are as effective or more effective and with less side effects for its treatment. This study compared treatment with antibiotic/glucocorticoid ear drops (hydrocortisone-bacitracin-
Study population: Children 1-10 years with otorrhea for up to 7 days in the Netherlands
Exclusion criteria included: T > 38.5 C, antibiotics in previous 2 weeks, PE tubes placed within 2 weeks, previous otorrhea in past 4 weeks, 3 or more episodes of otorrhea in past 6 months
Patient recruitment: ENT and PMD approached pt with PE tubes and they were told to call if otorrhea developed and a home visit would be arranged
Study type: open-label, pragmatic, randomized control trial
Primary outcome: Treatment failure defined as the presence of otorrhea observed otoscopically
Secondary outcome: based on parental diaries of symptoms, resolution and recurrence over 6 months
Results: After 2 weeks, only 5% of the ear drop group compared to 44% of the oral antibiotic group and 55% of the observation group still had otorrhea. There was not a significant difference between those treated with oral antibiotics and those that were observed. Otorrhea
lasted 4 days in the ear drop group compared to 5 days with oral antibiotics and 12 days with observation (all statistically significant).
Key differences: The antibiotic dosing and choice of ear drops are based on availability and local organism susceptibility.
Bottom line: For otorrhea in the presence of PE tubes, ear drops (with a non-aminoglycoside antibiotic and a steroid) may be more beneficial than oral antibiotics or observation.
Show References
Metformin is the first line medication for the treatment of type II diabetes. A rare complication of chronic metformin use is MALA.
- Incidence: 2-9 cases per 100,000 patients
- Mortality: 30-50%
The association between metformin accumulation and development of lactic acidosis is controversial as patients with suspected MALA experience concurrent illnesses such as sepsis/septic shock, tissue hypoxia, and/or organ dysfunction (especially renal failure).
- Greater than 90% of metformin (unchanged) is eliminated by the kidney.
- Metformin accumulation (from renal failure) leads to inhibition of complex I of the electron transport chain.1,2
- A case series of 66 patients MALA experienced severe lactic acidosis (pH: 6.91+ 0.18; lactate 14.36+ 4.9 mmol/L) and renal failure (Cr 7.24 + 3.29 mg/dL)3
- Prodromal GI symptoms in 77%
- Clinical findings at time of admission/presentation:
- AMS/coma: 57%
- Dyspnea/hyperventilation: 42%
- Hemodynamic shock: 39%
- Hypotension (SBP < 100 mmHg): 23%
- No correlation between lactate and metformin level.
- Risk factors
- Renal failure (metformin accumulation)
- Elderly population (higher mortality)
- Cardiac or respiratory insufficiency causing central hypoxia
- Sepsis/septic shock
- Liver disease
- IV contrast use (resulting in renal insufficiency)
- Treatment: emergent hemodialysis
Show References
Patient Positioning During Mechanical Ventilation
In any patient with acute respiratory failure, it is extremely important to consider patient positioning after initiating mechanical ventilation. Both ventilation (V) and perfusion (Q) of the lungs can be significantly altered by manipulating the way you position your patient.
- Routine Care: A good rule of thumb is to alays keep the patient's head of bed > 30 degrees whenever possible to maximize diaphragmatic excursion, increase lung expansion, and prevent downstream incidence of ventilator associated pneumonias.
- Lateral Decubitus Positioning: Severe unilateral lung disease may warrant alternative patient positiong.
- Good lung DOWN: In general, the good lung should be placed in the dependent position to improve V/Q matching.
- Good lung UP: Exceptions where the patient should be placed so the bad lung is in the dependent position include massive hemoptysis (prevent blood from filling the good lung), large pulmonary abscesses (prevent pus from filling the good lung), & unilateral emphysema (prevent hyperinflation)
- Reverse Trendelenburg: In the morbidly obese patient, or those who must remain flat in bed, a trick of the trade to achieve a pseudo-semirecumbent position is to utilize reverse trendelenburg to > 30 degrees.
Show References
Question
30 year-old presents with cough & fever. CXR shows mild right lower lobe pneumonia. The lung ultrasound of the right lower lobe is shown below. What's the diagnosis?
Show Answer
Show References
Ventricular Arrhythmias Associated with Myocardial Infarction
Therapeutic advances and management of acute myocardial infarction (AMI) has lead to a decreasing incidence of ventricular arrhythmias (VA)
VA remains a life-threatening occurrence after AMI, and all patients should be monitored closely during this vulnerable period
VA occurs more frequently inpatients with STEMI versus non-STEMI
Of those who develop VA’s, features associated with poor outcomes include:
· Late occurrence
· Sustained monomorphic VT
· Concurrent heart failure
· Cardiogenic shock
· Failure or lack of revascularization
Show References
Football helmets
A review of head and neck injuries from football from 1959 to 1963 found the rates of intracranial hemorrhage /intracranial death were 2-3X higher than the rates of cervical spine fracture/dislocation or cervical quadriplegia. In contrast, a study of football injuries from 1971 to 1975, revealed a dramatic reversal in rates. Cervical injuries now exceeded the rate of ICH by 2-4X.
A 66% reduction in ICH
A 42% reduction in craniocerebral deaths
A 204% increase in cervical spine fractures and dislocations
The shift was attributed to the modern football helmet, whose superior protection promoted “spearing” (headfirst tackling technique). Spearing involves hitting with the crown of the helmet leading to axial loading of the spine. Spearing accounted for 52% of the quadriplegia injuries from 1971 to 1975. Research by Joesph Torg, M.D., resulted in rule changes that led to an immediate 50% reduction in quadriplegia in NCAA football.
As a parent, coach or team physician, teach and enforce proper form and protect our young athletes.
- Over the last decade, multiple studies have shown that pain and sedation in children can be easily and quickly treated via intransal administration of traditional drugs.
- Inexpensive atomizers are used to quickly administer medications which are absorbed through the mucosal surface and rapidly delivered to the bloodstream and CNS with equivalent effects to intravenous administration.
- Considerations include using concentrated forms as volumes greater than 1mL per nostril may over-saturate the mucosa and drip out rather than be fully absorbed.
- The few side effects included cough, vocal cord irritation, and laryngospasm; but pre-treating with a single puff of lidocaine spray minimizes them and has been found to enhance sedative effects.
- Fentanyl, 2mcg/kg for pain
- Midazolam, 0.2 - 0.5mg/kg for sedation and antiepileptic.
- Ketamine and Dexmedetomidine have also been used with success, but standardized doses are still being studied.
Show References
In a single academic medical center, 273 poisonings required Pediatric ICU (PICU) admission over a 5-year period. This represented 8% of total PICU admissions during that time. Key findings include:
- Most poisonings occurred in patients either ≤3 years or ≥13 years.
- Most admissions were for less than 48 h and 41% were for less than 24 h. Mean PICU length of stay was 1.2 + 0.7 days.
- Analgesics and antidepressants were the most common substances.
- 27 patients received mechanical ventilation.
The majority of poisonings were non-fatal and required supportive care, close monitoring, and some specific treatment. Drug classes causing poisonings have changed to a higher percentage of opioids in younger patients and atypical antidepressants in adolescents.
Show References
In patients presenting to the ER with a TIA (transient ischemic attack), the classic teaching has been to calculate their ABCD2 score (age, blood pressure, clinical features, duration of episode and diabetes) to determine their risk of developing a stroke.
The problem is, a moderate-to-high ABCD2 score is sensitive (86%) but not specific (35%) for a stroke in 7 days.
The solution: Combining imaging data with the scoring system!
The presence of an acute infarct on a diffusion-weighted MRI (DWI) in a patient with an ABCD2 score of 4 or more carries the highest risk of stroke, at 14.9% at 7 days. On the other hand, a negative DWI predicts a 0-2% stroke risk at 7 days irrelevant of the ABCD2 score.