Search
281-300 of 555 results with category "Pediatrics"
Question
Q: What is wrong with this baby? And what Dx should you entertain?
Previously healthy 7d old presents after difficulty feeding, one episode of vomiting and now with intermittent apneic episodes.
Show Answer
Show References
Attachments
There are numerous different causes of pediatric hemorrhagic diarrhea. Consider a pediatric patient with bloody diarrhea as being at risk for developing hemolytic uremic syndrome. Most cases of hemolytic uremic syndrome are caused by O157:H7 strains of E Coli that release Shiga-like toxin from the gut. Systemic release of the toxin causes microvascular thromboses in the renal microvasculature. The characteristic microangiopathic hemolysis results with anemia, thrombocytopenia and peripheral schistocytes seen on laboratory studies, in addition to acute renal failure.
Antibiotics have been controversial in the treatment of pediatric hemorrhagic diarrhea due to concern that they worsen toxin release from children infected with E Coli O157:H7 and thus increase the risk of developing hemolytic uremic syndrome. Numerous previous studies have provided conflicting data regarding the true risk (1). A recent prospective study showed antibiotic treatment increases the risk (2). Most recommendations warn against using antibiotics to treat pediatric hemorrhagic diarrhea unless the patient is septic.
Bottom line: Avoid treating pediatric hemorrhagic diarrhea with antibiotics
Show References
Question
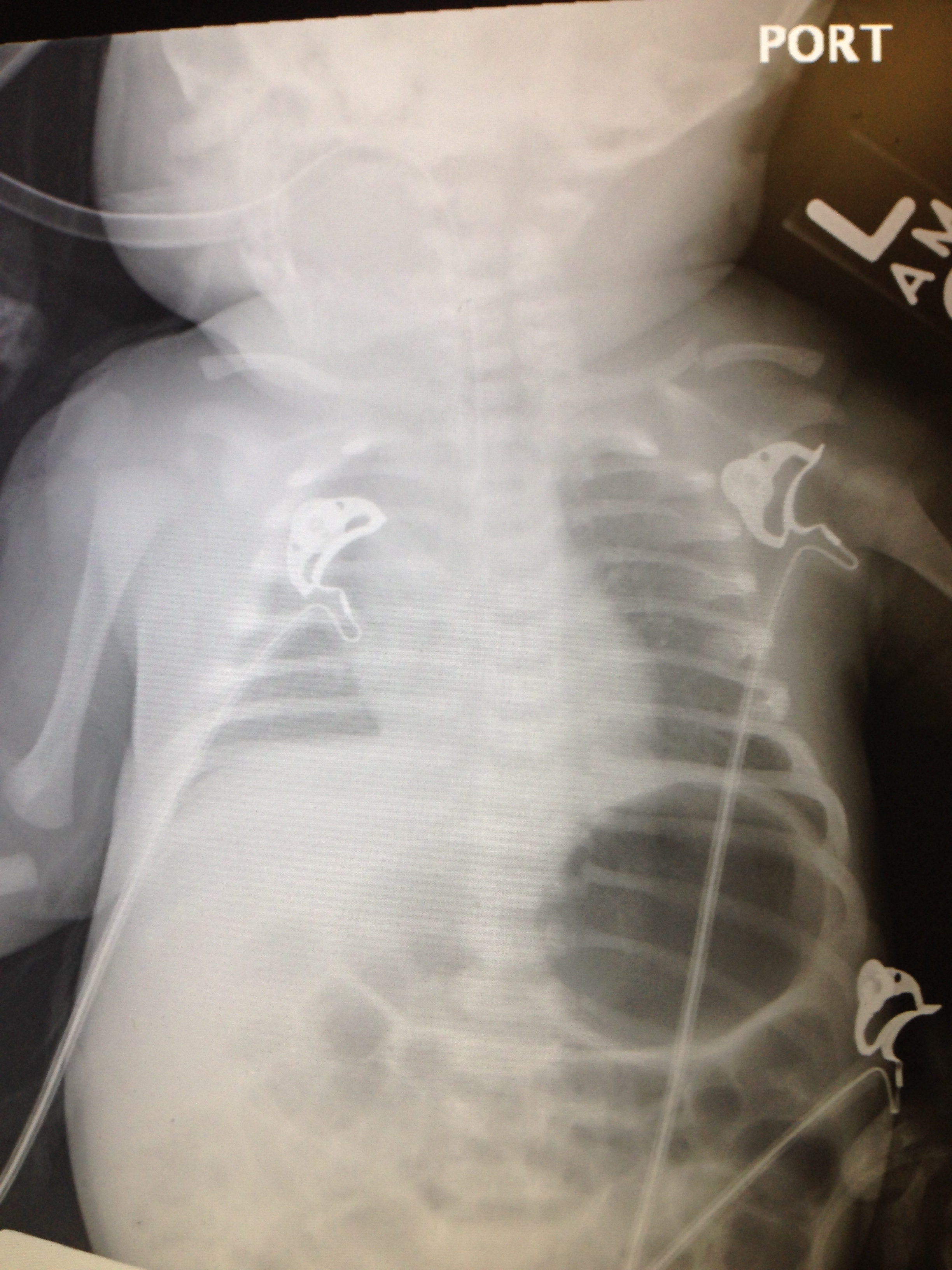
16 yo M with pleuritic right upper chest pain that started today. He is suffering from an asthma exacerbation currently in the setting of URI with cough. He is afebrile, tachycardic to 140-150s, respiratory rate 20, and sats 98% on room air. ECG was performed which incidentally diagnosed this patient WPW and he went for ablation as an outpatient. His chest x-ray showed:
Besides a bad day, what do we call this chest x-ray finding?
Show Answer
Show References
Attachments
The NEXUS criteria is widely applied to adults who present with neck pain due to trauma. While this study did include about 2000 pediatric patients, there were not enough young children to draw definitive conclusions. For more information on the evaluation of the cervical spine, see Dr. Rice's pearl from 9/7/12. A 2003 study piloted an algorithm for cervical spine clearance in children < 8 years.
Patients were spine immobilized if: unconscious, abnormal neurological exam, history of transient neurological symptoms, significant mechanism of injury, neck pain, focal neck tenderness or inability to assess based on distracting injury (extremity or facial fractures, open wound, thoracic injuries, or abdominal injuries), physical exam findings of neck trauma, unreliable exam due to substance abuse, significant trauma to the head or face, or inconsolable children.
When the 2 pathways (see attached) were implemented, there was a decrease in time to cervical spine clearance. There were no missed injuries in the study period prior to implementation of the pathway or once it was implemented. There was no significant difference in the amount of xrays, CT scans or MRIs.
Show References
Attachments
- The human enterovirus D68 is a rare virus closely related to the rhinovirus which causes the common cold. However, there have been recent outbreaks throughout the midwest and the areas are rapidly expanding.
- Mild symptom onset of rhinorrhea and cough rapidly progress to hypoxia and respiratory distress.
- Key features are the rapid progression, presence of wheezing even without a history of reactive airway disease, and typically an absence of consolidation on chest XR.
- Children under 5 years and those with asthma are at the greatest risk for respiratory failure.
- There are a limited number of labs in the US which test specifically for EV-D68. At UMMC, the Luminex respiratory virus panel can be ordered using the kit form which includes a flocked swab and viral transport media. Unfortunately, the panel does not differentiate between the closely related enterovirus and rhinovirus.
- There is no definitive cure, rather only supportive care and low-threshold for admission/observation for high risk patients.
Show References
6-7% of kids presenting with upper respiratory symptoms will meet the definition for ABS.
The American Academy of Pediatrics (AAP) reviewed the literature and developed clinical practice guideline regarding the diagnosis and management of ABS in children and adolescents.
The AAP defines ABS as: persistent nasal discharge or daytime cough > 10 days OR a worsening course after initial improvement OR severe symptom onset with fever > 39C and purulent nasal discharge for 3 consecutive days.
No imaging is necessary with a normal neurological exam.
Treatment includes amoxicillin with or without clauvulinic acid (based on local resistance patterns) or observation for 3 days.
Optimal duration of antibiotics has not been well studied in children but durations of 10-28 days have been reported.
If symptoms are worsening or there is no improvement, change the antibiotic.
There is not enough evidence to make a recommendation on decongestants, antihistamines or nasal irrigation.
Show References
- Only treat strep pharyngitis after confirmed via rapid antigen test or culture
- Remember the rapid antigen test has high specificity, but low sensitivity. All negative rapid antigen tests should be followed up with a confirmatory culture
- Traditionally, strep pharyngitis was treated with penicillin V, 250mg PO tid for children and 500 mg tid for adolescents. This was then changed to bid dosing.
- Now, consider treating with amoxicillin, 50mg/kg once daily (max 1000mg). Once daily dosing and better taste improve compliance
Show References
Up to 26% of patients with tympanostomy tubes (PE tubes) can suffer from clinically manifested otorrhea. This is thought to be the result of acute otitis media that is draining through the tube. Previous small studies suggested that antibiotic ear drops are as effective or more effective and with less side effects for its treatment. This study compared treatment with antibiotic/glucocorticoid ear drops (hydrocortisone-bacitracin-
Study population: Children 1-10 years with otorrhea for up to 7 days in the Netherlands
Exclusion criteria included: T > 38.5 C, antibiotics in previous 2 weeks, PE tubes placed within 2 weeks, previous otorrhea in past 4 weeks, 3 or more episodes of otorrhea in past 6 months
Patient recruitment: ENT and PMD approached pt with PE tubes and they were told to call if otorrhea developed and a home visit would be arranged
Study type: open-label, pragmatic, randomized control trial
Primary outcome: Treatment failure defined as the presence of otorrhea observed otoscopically
Secondary outcome: based on parental diaries of symptoms, resolution and recurrence over 6 months
Results: After 2 weeks, only 5% of the ear drop group compared to 44% of the oral antibiotic group and 55% of the observation group still had otorrhea. There was not a significant difference between those treated with oral antibiotics and those that were observed. Otorrhea
lasted 4 days in the ear drop group compared to 5 days with oral antibiotics and 12 days with observation (all statistically significant).
Key differences: The antibiotic dosing and choice of ear drops are based on availability and local organism susceptibility.
Bottom line: For otorrhea in the presence of PE tubes, ear drops (with a non-aminoglycoside antibiotic and a steroid) may be more beneficial than oral antibiotics or observation.
Show References
- Over the last decade, multiple studies have shown that pain and sedation in children can be easily and quickly treated via intransal administration of traditional drugs.
- Inexpensive atomizers are used to quickly administer medications which are absorbed through the mucosal surface and rapidly delivered to the bloodstream and CNS with equivalent effects to intravenous administration.
- Considerations include using concentrated forms as volumes greater than 1mL per nostril may over-saturate the mucosa and drip out rather than be fully absorbed.
- The few side effects included cough, vocal cord irritation, and laryngospasm; but pre-treating with a single puff of lidocaine spray minimizes them and has been found to enhance sedative effects.
- Fentanyl, 2mcg/kg for pain
- Midazolam, 0.2 - 0.5mg/kg for sedation and antiepileptic.
- Ketamine and Dexmedetomidine have also been used with success, but standardized doses are still being studied.
Show References
Show References
Mental health-related visits account for 1.6–6% of ED encounters. Patients with acute psychosis are often brought to the ED for clearance prior to psychiatric evaluation. Is this necessary?
Background: Several adult studies have shown that only 0–4% of patients with isolated psychiatric complaints have organic diagnoses requiring urgent treatment. Routine ED laboratory testing in adults is low yield still, with one study identifying abnormalities in only 2 of 352 patients—both mild hypokalemia. A pediatric study found that 207 of 209 patients were medically cleared.
This study was a retrospective review of pediatric psychiatric patients presenting to a an urban California hospital. They examined 798 patients who had an involuntary psychiatric hold placed by a psychiatric mobile response team.
- 72 (9.1%) were determined to require medical screening (based on patient complaints).
- Only 35 (4.4%) holds were found to require further medical care prior to psychiatric hospitalization.
- Total charges for laboratory assessments, secondary ambulance transfers and wages for sitters were $1,241,295 or US$17,240 per patient requiring a medical screen.
- Patients were in the ED for an average of 7 h with a cumulative time of 5538 hours.
The authors concluded that few pediatric patients brought to the ED on an involuntary hold required a medical screen and perhaps use of basic criteria in the prehospital setting to determine who required a medical screen (altered mental status, ingestion, hanging, traumatic injury, unrelated medical complaint, sexual assault) could have led to significant savings.
Show References
Scabies is considered by the WHO to be one of the main neglected diseases with approximately 300 million cases worldwide each year. One third of cases of scabies seen by dermatologists are in kids less than 16 years old. The belief had been that presentation varies by age. One French study reported a first time miss rate of more than 41% and an overall diagnostic delay of 62 days.
A prospective, multi center observational study of patients with confirmed scabies sought to determine common phenotypes in children. All patients were seen by dermatologists in France and administered standard questionnaires. They were divided into 3 age groups, <2 years, 2-15 years and > 15 years. 323 patients were included.
The study found that:
-infants were more likely to have facial involvement and nodules, especially on the back and axilla
-relapse was more common in < 15 year olds - this was hypothesized to be due to poor compliance with treatment to the head
-family members with itch, or planter or scalp involvement were independently associated with diagnosis of scabies in kids < 2 years
-burrows were seen in 78%, nodules in 67% and vesicles of 43% of patients (see photo)
-itching was absent in up to 10% of patients
Bottom line: Have a high suspicion for scabies in any rash.
Show References
Attachments
- Male infants are routinely given a sweet solution prior to circumcision for analgesia.
- Michelis and Hoyle recently published a great review of the possible use of sweet solutions in the ED for pediatric patients.
- Pediatric patients often undergo painful, but rather routine procedures in the ED such as IV and urinary catheter placement, venipuncture, and lumbar punctures.
- More often than not, however, they are not provided analgesia prior to these procedures.
- It is believed that repetitive early pain events lead to anxiety and other behavioral disorders while also decreasing pain tolerance.
- In children less than 12 months, consider giving a sweet solution (2mL of 24% sucrose) 2 minutes before any painful procedure.
- Multiple studies indicate decreased pain as measured by significantly reduced crying times.
- It's cheap, safe, and works!
Show References
Show References
Hot off the press! Pediatrics March 2014 just published results of a meta-analysis that compared 1 or 2 dose regimens of Dexamethasone versus 5 day course of Prednisone/Prednisolone for management of acute asthma exacerbations in pediatric patients. The results showed that Dexamethasone was as efficacious as the longer course of Prednisone. End points used were return trips to the emergency department and hospital admissions. On further review of the literature, parents tend to prefer the shorter duration of therapy with Dexamethasone. Also, there is less vomiting associated with Dexamethasone. There have been several articles published that show Dexamethasone is more cost-effective than Prednisone. Bottom line: consider giving single dose of Dexamethasone in the ER and then sending patient home with 1 additional dose.
Show References
Passive leg raise (PLR) has been studied in adults as a bedside tool to predict volume responsiveness (see previous pearls from 5/7/13 and 6/17/2008). Can this be applied to children?
A single center prospective study looked at 40 intensive care patients ranging in age from 1 month to 12.5 years. They used a noninvasive monitoring system that could measure heart rate, stroke volume and cardiac output. These parameters were measured at a baseline, after PLR, after another baseline and after a 10 ml/kg bolus.
Overall, changes in the cardiac index varied with PLR. However, there was a statistically significant correlation in children over 5 years showing an increase in cardiac index with PLR and with a fluid bolus.
Bottom line: In children older then 5 years, PLR can be a quick bedside tool to assess for fluid responsiveness, especially if worried about fluid overload and in an under served area.
Show References
Inborn errors of metabolism (IEM) are rare, each typically affecting 1 in 5000 to 1 in 100,000 children, BUT collectively these disorders are more common because there are so many. If you are lucky…when they present to the ED they come with a letter from Dr. Greene (our world renowned metabolic geneticist) detailing exactly what to do. The rest of the time…you are on your own. Think about IEM in any neonate or child with history of feeding difficulties, failure to thrive, recurrent vomiting, unexplained altered mental status and/or acidosis. Pay particular attention to feeding difficulties that appear with changes in diet: switch from soy to cow’s milk formula (galactose), addition of juice or fruit or certain soy formulas (fructose), switch from breast milk to formula or foods (increased protein load), and longer fasting periods from sleeping or illness.
For this pearl, we will focus on primary hyperammonemia from an enzymatic block in ammonia metabolism within the urea cycle. It is important to remember that secondary hyperammonemia can result from metabolic defects such as organic acid disorders, fatty acid oxidation disorders, drugs that interfere with urea cycle, or severe liver disease. Amino acids liberated from excess protein breakdown (stress of newborn period, infection, injury, dehydration, surgery, or increased intake) release nitrogen which circulates as ammonia. Ammonia is then converted to urea via the urea cycle and excreted in the urine. With urea cycle defects (UCD) there is an enzymatic block in the cycle that results in accumulation of ammonia which has toxic effects on the CNS especially cerebral edema. The most common UCD is ornithine transcarbamylase deficiency followed by argininosuccinic academia, and citrullinemia.
Clinical presentation includes poor feeding, lethargy, tachypnea, hypothermia, irritability, vomiting, ataxia, seizures, hepatomegaly, and coma. Hyperammonemic crises in neonates mimic sepsis! If you think about an IEM in your differential, send plasma ammonia (1.5 mL sodium-heparin tube on ice STAT), plasma amino acids, and urine organic acids. Other helpful labs include blood gas, CMP, urinalysis (looking at ketones), lactate, plasma acylcarnitines, and newborn screen if not already sent. Plasma ammonia is a direct index of CNS toxicity and important to follow for acute management. Serum level > 150 in sick neonate or > 100 in sick infant/child is concerning for IEM. The presence of hyperammonemia and respiratory alkalosis suggest urea cycle defect. The presence of metabolic acidosis and hyperammonemia suggests organic acid disorder.
Immediate treatment of hyperammonemia is critical to prevent neurologic damage. Cognitive outcome is inversely related to the number of days of neonatal coma caused by the cerebral edema.
1. Stop all protein intake! You need to stop catabolism.
2. Start D10 at 1.5 times maintenance rate with GIR at least 6-8. Start intralipids 1-3g/kg/day when able (typically in the ICU after central line placed).
3. Give ammonia scavenger medications sodium benzoate and sodium phenylacetate. These are available commercially as Ammonul.
a. 0-20kg: 2.5mL/kg IV bolus over 90 min followed by same dose as 24 hr infusion
b. >20kg: 55 mL/m2 IV bolus over 90 min followed by same dose as 24 hr infusion
4. HEMODIALYSIS! Dialysis is the most effective way to remove ammonia and should be done when level > 300. The decision to hemodialyze is crucial in preventing irreversible CNS damage; when in doubt in the face of elevated ammonia, HEMODIALYZE!
- Much attention has been paid towards early goal-directed therapy for sepsis in adult ED patients, but there has not been as much consideration for the pediatric ED patient.
- R-C analyses and M&M reviews have consistently identified system difficulties recognizing sepsis in children, especially cases of compensated shock, and subsequent management.
- Protocols beginning in triage to recognize abnormal vital signs, followed by timely execution of interventions especially antibiotic and fluid administration are worthwhile to reduce overall morbidity and mortality.
- Protocols should include 3 major goals:
- Triage vital signs adjusted for age, and corrected heart rate for pyrexia to recognize sepsis.
- Obtain vascular access within 5 minutes followed by a 20mL/kg bolus of IV fluids administered within 15 minutes in cases of volume depletion.
- Antibiotic administration within 30 minutes.
Show References
Show References
Head lice infestation is a common problem in the United States with treatment costs estimated at 1 billion dollars and cases affecting millions of children each year. Many of these children present to the ED for care...lucky us! Traditional therapies containing permethrin and pyrethrins are having increased rates of treatment failure likely secondary to increasing resistance and medication noncompliance. The typical first line agents require multiple doses. There are safety concerns regarding therapies that contain malathion and lindane in children. Is there another option? Topical ivermectin 0.5% lotion applied to scalp in a single dose has been shown to be effective and safe for treatment of head lice infestation in children older than 6 months. It was FDA approved at the end of 2012. Considerations include cost. Sklice lotion is expensive!
The NEJM article was considered an "editors pick" by the AAP as one of the best articles of 2012-2013.