Search
21-40 of 213 results with category "Trauma"
Looking at a national database, this study concluded the use of low titer O whole blood during trauma resuscitations was increasing at level one centers but not at level 2 and 3 centers. Is this a representation of the national blood supply as whole blood is harder to stock? We need to understand this trend to assure equal and appropriate care to trauma patients across the country.
Show References
Another study, this one from New Zealand, showing older trauma patients with similar injury severity score had less trauma team activations and higher mortality.
Show References
When compared to saline(!) trauma patients with a high injury severity score who received ketamine via pca for pain control had better quality of life indicators at 1,3, and 6 months post injury.
Show References
In a single level 1 trauma center there were 274 patients age over 55 evaluated for falls in a one year retrospective period. Their blood toxicology was reviewed for presence of alcohol, opioids, benzodiazepines and cannabinoids. The authors found:
“detection rates were 21.2% for opioids, 18.6% for ethanol, 13.9% for benzodiazepines, and 9.1% for cannabinoids. Injuries identified included 16.4% spinal fractures, 9.5% extremity fractures, 7.7% hip/thigh/pelvic fractures…In this study, nearly 20% of adults 55+ presenting for fall-related trauma recently used substances that impair psychomotor function.”
An area for injury prevention research and intervention would be to screen patients over age 55 for substance use, consider prescribing patterns in this age group (benzodiazepines) , and discuss with patients fall risk avoidance.
Show References
A case report on use of the abdominal aortic and junctional tourniquet in a 27 year old female with hemorrhagic shock secondary to a pelvic fracture after a 10 meter fall demonstrated improved blood pressure and stabilized vasopressor use prior to operative intervention. This device has been used in battlefield situations, however very few reports of civilian use exist. Much more data is needed, however, it is a device to be aware of for future use.
Show Additional Information

Show References
In a metanalysis of studies looking at intercranial hemorrhage in fall patients older than 65 years, the following were unadjusted odds ratio risk factors for finding an ICH in this patient population:
suspected open or depressed skull fracture , signs of basal skull fracture ), reduced baseline Glasgow Coma Scale score , focal neurologic signs , seizure , vomiting , amnesia , loss of consciousness , headache ), external sign of head trauma , male sex , chronic kidney disease , preinjury single antiplatelet , and dual antiplatelet medication .
Preinjury anticoagulant was not a significant risk factor.
When looking at adjusted odds rations only focal neurologic signs , external sign of head trauma , loss of consciousness , and male sex were found to be associated with intercranial hemorrhage.
Show References
An English study describes 30 patients that jumped from a single bridge of 30 meters (98 feet) over the course of 12 years. Twenty six landed in the water. The injury pattern for those landing in water was described as “Hypothermia was the most common presentation (n = 23), followed by pneumothoraces (n = 14), rib fractures (n = 10), thoracic vertebral fractures (n = 9) and lung contusions (n = 8). Lower water temperatures at the time of the incident (p = 0.008) and lower patient body temperatures on arrival to hospital (p = 0.002) were significantly associated with increased 30-day mortality.”
The small group landing on land had more pelvic and extremity fractures than the water group and none had hypothermia.
Remember to start aggressive rewarming in patients who fall into water!
Show References
This small study from South Africa shows stab wounds to the chest with a pneumothorax less than 0.5 cm that were managed conservatively had completely resolved on 12 hour repeat chest X-ray. This could facilitate earlier discharge of these patients. It also supports conservative (non-tube placement) approach to asymptomatic small pneumothoraces from stab wounds.
Show References
A reminder from a recent position paper on pelvic trauma that we should not be doing stability testing to evaluate pelvic trauma
“EMS clinicians should recognize the challenges in accurately identifying pelvic fractures by physical exam alone. Manual stability testing of the pelvis is neither sensitive nor specific and may cause harm.”
Show References
Much has been written about the benefits of prehospital blood transfusion for traumatic hemorrhage. Can this success be ascribed to non-traumatic hemorrhage as well? This small study (50 patients over 10 years!) says there were improvements in patient physiology (shock index) for those patients receiving blood for GI bleed, etc. Much more research is needed however this could be a beneficial practice in the future.
Show References
This systematic review found improved pain scale at 15 and 120 minutes in 495 patients who received nebulized ketamine. Dosing at 0.75 mg/kg was as effective as 1.5 mg/kg and the nebulized ketamine was non-inferior to IV morphine and ketamine with fewer side effects.
Show References
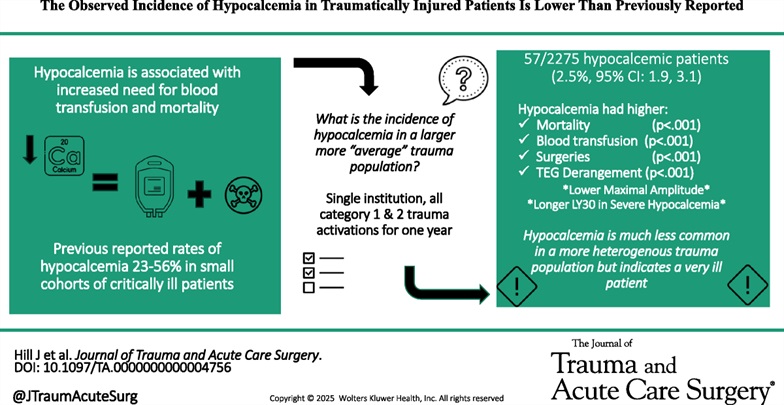
Previous small studies had put the prevalence of hypocalcemia in trauma patients at 23-56%. This single center study of 2200 patients looked at prevalence and outcome and found a much lower prevalence however worse outcomes than those who were not hypocalcemic.
Show References
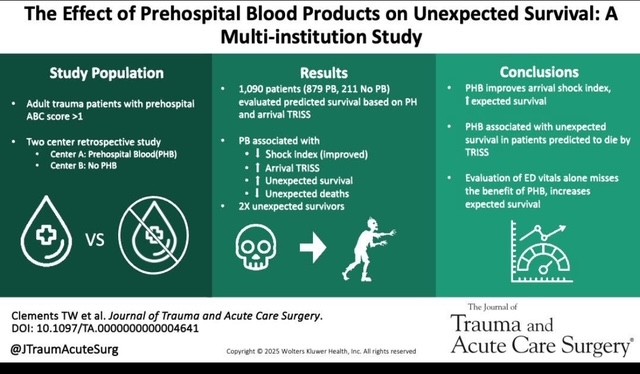
This study demonstrated that administration of prehospital blood to trauma patients lead to a higher rate of survival in patients whose initial ED vital signs or pre-hospital shock index would have predicted death.
Show References
This review article reminds us that circulation needs to be prioritized over airway in trauma patients. This means bleeding control (pressure on wound, tourniquet, surgery/IR intervention), correcting tension pneumothorax, correcting pericardial tamponade, as well as resuscitation to return physiologic homeostasis (blood products, vasopressors where needed, warm the patient, etc.) before intubation. Altered mental status/low GCS may be due more to hypoperfusion than neurologic injury. Correcting the hypotension may alleviate that need to intubate.
Show References
In 252 mild traumatic brain injury patients seen at 3 level I centers that were given the Rivermead Post Concussion Symptoms Questionnaire within 24 hours of arrival, 3 month post concussive symptoms were significantly correlated with their score on the questionnaire. This questionnaire take 3 minutes to complete. This may be helpful in prognosticating who will have post-concussive symptoms and who will need additional follow up.
Show References
This group looked at 88 patients intubated for penetrating neck injury and found 95% received neuromuscular blocking agents, 73% were intubated using a bougie, and 95% were intubated on first pass.
The authors concluded; “Rapid sequence intubation with bougie use was an effective default approach to definitive airway management in ED patients with penetrating neck trauma.”
Show References
These authors followed 250 consecutive trauma activation patients over a one year period. In hospital elevated blood pressure and glucose level correlated with a new diagnosis of hypertension and diabetes respectively over that 1 year time line. Some of these patients also had a new diagnosis of HIV, substance use disorder and hepatitis C. Using their contact with the health system due to trauma can be a way to screen for undiagnosed medical problems such as diabetes and hypertension. Assuring outpatient follow up for these patients will have an effect on their long term morbidity and mortality.
Show References
In a German study comparing one EMS jurisdiction which used IV paracetamol (acetaminophen) in combination with nalbuphine (Nubian, opiate agonist/antagonist) to another jurisdiction which used piritramide (synthetic opioid similar to fentanyl) for prehospital traumatic pain, the combination worked better to decrease pain on a numerical scale. There were no differences in typical safety measures.
The use of an antagonist/agonist theoretically could precipitate withdrawal in non-opiate naive patients and could influence in hospital analgesic choices. The literature on this is mixed.
This study offers further evidence of the efficacy of multi-modal pain control, the feasibility of paramedics using IV paracetamol and the possibility of using rapid onset opioid agonist/antagonist in the prehospital setting.
Show References
Another paper emphasizing care for brain injured patients should include:
-pre-intubation preoxygenation to avoid hypoxia
-pre-intubation avoid extremes in blood pressure (hypotension kills)
-use hemodynamically neutral induction agents such as ketamine or etomidate
-post intubation target eucapnia on the ventilator. (do not aim for low CO2)
-post intubation maintain adequate sedation to avoid increased intercranial pressure
Show References
This paper reminds us older patients have higher mortality and worse outcomes overall if their injury includes a head injury. Any mechanism that results in head injury, including fall from standing, has a higher potential for death, disability, and long term cognitive decline in older patients. Triaging these patients to trauma centers can lead to better outcomes. The difficulty is knowing which patients to send to trauma centers vs. emergency departments. The authors write:
"clinicians should consider transporting to a trauma center in geriatric patients with head trauma, if feasible. However, given the frequency with which head injury occurs, transportation to a trauma center for all patients with head trauma is likely to overwhelm EMS systems and hospitals. Unfortunately, the existing literature does not delineate the subset of patients whose condition will benefit from this evaluation . Given these considerations, we recommend EMS clinicians consider abnormal mental status, presence of anti-coagulation, and loss of consciousness as considerations to transport to a trauma center in cases where the need for trauma center evaluation is not clear.”