Search
221-240 of 879 results with category "Critical Care"
Norepinephrine is widely considered the first-line vasopressor for patients in septic shock. Vasopressin is often added to norepinephrine in patients requiring escalating doses, but when to add vasopressin, and what exactly the benefit is (as opposed to just further titrating up the norepinephrine) remain unclear. Given the limited evidence for a patient-oriented benefit and the increasing cost of vasopressin, some centers are becoming more judicious in the use of vasopressin. A systematic review in AJEM October 2021 examined the literature on early (< 6 hours of diagnosis) addition of vasopressin to the management of septic shock patients, compared to either no vasopressin or starting it after 6 hours.
Improved with early vasopressin: Need for renal replacement therapy (RRT; secondary outcome)
No difference: mortality, ICU length of stay, hospital length of stay, new onset arrhythmias
Bottom Line: When, and if, to start vasopressin in patients requiring escalating doses of norepinephrine remains controversial. Based on the prior VASST trial, many providers will start vasopressin when norepi doses reach ~ 5-15 mcg/min (approx 0.1-0.2 mcg/kg/min), but there remains limited data to support this practice, and either starting vasopressin or continuing to titrate the norepinephrine as needed are both reasonable approaches in most patients.
Show References
Refractory Anaphylaxis
- Refractory anaphylaxis is defined as anaphylaxis that does not respond to at least 2 doses of 300 mcg of epinephrine given IM into the anterolateral thigh.
- Refractory anaphylaxis can be due to several factors including patient comorbidities, delayed diagnosis, delayed epinephrine administration, or concomitant beta-blocker or ACE-inhibitor medication use.
- Consider the following treatments in patients with refractory anaphylaxis, persistent hypotension, and shock:
- Aggressive IVF resuscitation - patients may need up to 7L of IVFs
- Epinephrine infusion (1-10 mcg/min) to target a MAP of 65 mm Hg
- Glucagon (1-5 mg via slow IV push) for those taking a beta-blocker and who fail to respond to epinephrine
- Norepinephrine, vasopressin, angiotensin II, methylene blue, or dobutamine can be administered with epinephrine for persistent hypotension.
- VA-ECMO - though there is no prospective evidence on the use of ECMO in anaphylaxis.
Show References
RECAP: RECOVERY trial is a large, randomized, open label, adaptive trial studying different treatments on COVID-19. Most well known is the use of dexamethasone which reduced mortality by 1/3 in COVID patients requiring mechanical ventilation and by 1/5 in those requiring oxygen, with no benefit on those patients not requiring oxygen.
They recently published results in the Lancet on the use of tocilizumab.
Population:
- Up to 21 days after main randomization, regardless of treatment, RECOVERY trial patients with progressive COVID-19 were eligible for tocilizumab.
Inclusion:
- April 23rd 2020 to Jan 24th 2021-- 21,550 patients with hypoxia (<92% on RA or requiring O2), systemic inflammation (CRP > 75 mg/L) eligible for standard care or standard care plus toci 400-800 mg (dosing based on weight), second dose 12-24 hours later if no improvement
Outcomes:
- Primary outcome 28 day mortality followed by:
- Hospital discharge within 28 days
- Rate of mechanical ventilation
Results:
- 621 (31%) tocilizumab patients and 729 (35%) of usual care patients died within 21 days (RR 0.85, p=0.0028). Consistent even in those receiving steroids (83%).
- Tocilizumab group more likely to be discharged from the hospital, less likely to receive invasive mechanical ventilation (35% vs 42%).
Conclusion:
- Tocilizumab improved survival and other clinical outcomes- by 1/3 for those on simple oxygen, and by ½ for those receiving invasive mechanical ventilation.
- Added to the additional benefit of steroids.
- Findings support the earlier REMAP-CAP trial on the effectiveness of tocilizumab for ICU COVID patients
Show Additional Information
Show References
Background:
Cardiac arrest from massive pulmonary embolism (PE) can be up to 90% (1). A recent systemic review evaluated the efficacy of Venoarterial-Extracorporeal Membrane Oxygenation (VA-ECMO) for PE-related cardiac arrest.
Results:
The authors screened 1115 articles and included 77 articles, including gray literature. The authors performed a quantitative analysis of a total of 301 patients.
Overall, 183/301 (61%) patients survived to hospital discharge, a significant improvement from 90%.
Patients who were cannulated during chest compression were associated with 7x higher odds of death (OR, 6.84; 95% CI, 1.53–30.58; p = 0.01), compared to those who were cannulated after ROSC. However, cannulation in the ED was not associated with improved outcomes, compared with other cannulation site.
No increased risk of death among patients who received tPA prior to VA-ECMO vs. those who did not (OR, 0.78; 95% CI, 0.39–1.54; p = 0.48).
Patients whose age > 65 years of age were associated with 3X risk of death, compared to those with age < 65 years (OR, 3.56; 95% CI, 1.29–9.87; p = 0.02).
Take-home points
Please consider “early” VA-ECMO for eligible patients who have cardiac arrest from massive PE. However, it will take great convincing to push the PERT team to cannulate for VA-ECMO while the patient is still receiving chest compression.
Show References
Background:
Cardiac arrest from massive pulmonary embolism (PE) can be up to 90% (1). A recent systemic review evaluated the efficacy of Venoarterial-Extracorporeal Membrane Oxygenation (VA-ECMO) for PE-related cardiac arrest.
Results:
The authors screened 1115 articles and included 77 articles, including gray literature. The authors performed a quantitative analysis of a total of 301 patients.
Overall, 183/301 (61%) patients survived to hospital discharge, a significant improvement from 90%.
Patients who were cannulated during chest compression were associated with 7x higher odds of death (OR, 6.84; 95% CI, 1.53–30.58; p = 0.01), compared to those who were cannulated after ROSC. However, cannulation in the ED was not associated with improved outcomes, compared with other cannulation sites.
No increased risk of death among patients who received tPA prior to VA-ECMO vs. those who did not (OR, 0.78; 95% CI, 0.39–1.54; p = 0.48).
Patients whose age > 65 years of age were associated with 3X risk of death, compared to those with age < 65 years (OR, 3.56; 95% CI, 1.29–9.87; p = 0.02).
Take-home points
Please consider “early” VA-ECMO for eligible patients who have cardiac arrest from massive PE. However, it will take great convincing to push the PERT team to cannulate for VA-ECMO while the patient is still receiving chest compression.
Show References
Supplemental oxygen therapy is frequently required for patients presenting with acute respiratory distress and COPD exacerbation. Over-oxygenation can derail compensatory physiologic responses to hypoxia,1 resulting in worsening VQ mismatch and, to a lesser degree, decreases in minute ventilation, that cause worsened respiratory failure.
The 2012 DECAF (Dyspnea, Eosinopenia, Consolidation, Acidaemia, and Atrial Fibrillation) score was found to predict risk of in-hospital mortality in patients admitted with acute COPD exacerbation.2,3 Data from the DECAF study’s derivation and external validation cohorts were examined specifically to look at outcome associated with varying levels of oxygen saturation.
- 1027 patients from 6 UK hospitals receiving supplemental oxygen at admission
- Lowest in-hospital mortality seen in the 88-92% cohort
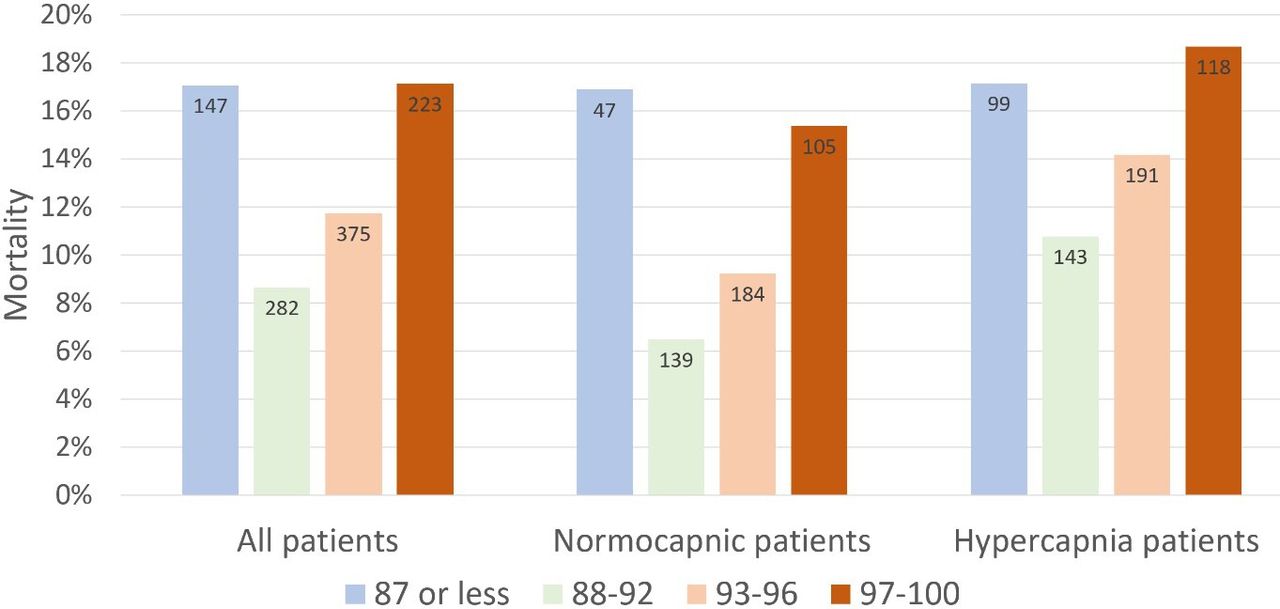
- Adj OR for in-hospital mortality in ≥97% vs 88-92% group: 2.97 (95% CI 1.58-5.58, p=0.001)
- Adj OR for in-hospital mortality in 93-96% vs 88-92% group: 1.98 (95% CI 1.09-3.60, p=0.025)
- Surprisingly, mortality risk seen more in normocapnic than hypercapnic patients
- Association between admission SpO2 and mortality persisted after adjusting for baseline risk and disease severity using the DECAF and NEWS 2 score
Bottom Line
In patients presenting to the ED with acute COPD exacerbation requiring oxygen supplementation, a target oxygen saturation of 88-92% is associated with the lowest in-hospital mortality, and higher oxygen saturations should be avoided independent of patients' PCO2 levels.
Show References
Two items from the recent INSPIRATION trial UMEM pearl were very well pointed out by our own Dr. Michael Scott and require clarification. Thank you to all our readers for their close attention, and please know that we always appreciate you reaching out with questions/comments.
- Dosing Correction - The "standard-dose" prophylactic dosing of enoxaparin in this trial was 40 milligrams/day. Please excuse the error in the prior post stating 40 mg/kg/day (we will revise the post). Standard dosing of enoxaparin for DVT/VTE prophylaxis was a flat 40 mg/day, and was not weight based.
- Major Bleeding - While the difference in major bleeding (2.5% vs 1.4%) was relatively small, this endpoint DID NOT meet non-inferiority. In other words, the study appeared to detect a statistically significant difference in major bleeding between the dosing regimens. Given that this is a single study and there are concerns with this finding (the authors themselves describe this as "exploratory"), I would interpret this with caution, but this supports the very intuitive notion that the intermediate (higher) dose regimen of enoxaparin would be associated with more bleeding than the standard dose regimen.
COVID-19 is generally regarded as a hypercoagulable state, and the role of pulmonary emboli and other VTE in COVID remains unclear. As a result, how to optimally provide prophylactic anticoagulation in COVID-19 patients who are not known to have VTE has been a point of debate.
The INSPIRATION trial looked at 600 patients admitted to academic ICUs in Iran, and compared what is often-referred to as "intermediate-dose" prophylaxis (in this case 1 mg/kg daily of enoxaparin) to standard dose prophylaxis (40 mg/day of enoxaparin). The study utilized a combined endpoint of venous thromboembolism, arterial thromboembolism, need for ECMO, or mortality. As a reminder, composite endpoints can skew results. However, the dose and type of anticoagulant chosen is similar to many academic centers around the world, and pharmacy guidelines often recommend providing this type of "intermediate-dose" prophylaxis in COVID-19 patients, sometimes based on clinical status, d-dimer or other coagulation-related patient-data. As with many things with COVID-19, this practice is based on limited data.
There was no significant difference between groups in the primary outcome (45.7% in intermediate ppx group vs 44.1% in standard group), and while safety outcomes were similar (major bleeding in 2.5% in the intermediate ppx group vs 1.4% in standard group), the intermediate regimen failed to demonstrate non-inferiority to the standard regimen for major bleeding.
Intermediate vs standard-dose ppx was similar in this study with a small, but statistically significant increase in major bleeding in the intermediate-dose group.
Bottom Line: Although this study had methodologic flaws and there are external validity concerns, the INSPIRATION trial supports the notion that standard dose (e.g. 40 mg/g/kg/day enoxaparin) and intermediate-dose (e.g. 1 mg/kg/day enoxaparin) VTE prophylaxis are equivalent in critically ill COVID-19 patients who do not already have a known VTE in terms of preventing negative VTE outcomes. Intermediate-dose may be associated with increased bleeding. As more critically ill patients require ED boarding, the dose of VTE prophylaxis may remain controversial, but the need to start it remains an important consideration.
Show References
Improving Compliance with Lung-Protective Ventilation
- Approximately 250,000 ED patients are intubated and receive mechanical ventilation each year in the United States.
- While emergency physicians understand the importance of providing lung-protective ventilation, current studies demonstrate that more than 40% of ED patients are placed on initial tidal volumes > 8 ml/kg of predicted body weight (PBW).
- In many cases, this may be due to the inaccurate estimation of patient height when determining PBW.
- In a recent single-center study, Tallman and colleagues evaluated a quality improvement intiative, whereby respiratory therapists were provided with a tape measure and an EHR BPA that reminded them to measure the patient's height for PBW.
- In this study, these simple, low-cost interventions significantly increased compliance with lung-protective ventilation.
- Take Home Pearl: Be sure to measure your intubated patient to accurately determine PBW and set the correct tidal volume.
Show References
The PARAMEDIC2 trial in NEJM 2018 studied the outcomes of the use of epinephrine in outside hospital cardiac arrest (OHCA) on survival and neurological outcome.
Methods: Conducted in Britain, randomized 8007 patients to receive either epinepherine 1mg (n=4012) or placebo (n=3995) as part of standard CPR for out-of-hosptial arrest. Their primary outcome was survival at 30 days and their secondary outcomes included length of stay as well as neurological outcomes at 30 days and 3 months.
Results: The epinepherine group had improved survival to hospital admission (23% vs. 8%), at 30 days (3.2% vs. 2.4%) or at 3 months (3% vs. 2.2%). Favourable neurological outcomes, however, had no statistical difference at both hospital discharge and at 3 months.
Bottom line: Epinephrine improves ROSC, though with poor neurological outcomes.
Important facts:
- Demographics: Mean age 69 years, 35% female
- Initial cardiac rhythm: shockable 19%, Non-shockable 78%, Undetermined 2%
- Cause of Cardiac Arrest: Medical 91% Traumatic 2%, Drowning 0.2%, substance overdose 2%, Asphyxia 3%, missing data 2%
- Witness of cardiac arrest: none 37%, Paramedic 11%, Bystander 50%, missing data 1%
- CPR Performed by: Paramedic 11%, bystander 59%, missing data 2%
- Time from: emergency call to ambulance arrival 6min, emergency call to administration of drug 22 min, arrival to ambulance departure 50 min
Recently, a follow up of the PARAMEDIC2 trial was completed in Resuscitation.
They reported long-term survival, quality of life, functional and cognitive outcomes at 3, 6 and 12-months.
Results: At 6 months, 78 (2.0%) of the patients in the adrenaline group and 58 (1.5%) of patients in the placebo group had a favourable neurological outcome (adjusted odds ratio 1.35 [95% confidence interval: 0.93, 1.97]). 117 (2.9%) patients were alive at 6-months in the adrenaline group compared with 86 (2.2%) in the placebo group (1.43 [1.05, 1.96], reducing to 107 (2.7%) and 80 (2.0%) respectively at 12-months (1.38 [1.00, 1.92]). Measures of 3 and 6-month cognitive, functional and quality of life outcomes were reduced, but there was no strong evidence of differences between groups.
Bottom line: Epinephrine improves survival at 12 months, but poor neurological outcomes remain.
Show Additional Information
Show References
Background:
The association between time intervals of ED antibiotic administration and outcome has been controversial. While single studies showed there was increased mortality associated with delayed antibiotic administration (1-3). A meta-analysis of 13 studies and 33000 patients showed that there was no mortality difference between septic patients receiving immediate Abx (< 1 hour) vs. those receiving early abx (1-3 hours) (4).
Since delay in recognition of sepsis (defined as ED triage to Abx order) and delay in antibiotics delivery (Abx order to administration) contribute to total delay of Abx administration, a new retrospective study (3) attempted to investigate the contributions of either factor to hospital mortality.
Results:
The study used generalized linear mixed models and involved 24000 patients.
For All patients and outcome of hospital mortality:
Recognition delay (ED triage to Abx order): OR 2.7 (95% CI 1.5-4.7)*
Administration delay at 2-2.5 hours (Abx order to administration): OR 1.5 (1.1-2.0)
These results was associated with non-statistical significance in patients with septic shocks.
Conclusion:
Delayed recognition of sepsis was associated with higher hospital mortality. Longer delay of abx administration was also associated with increased risk of hospital mortality.
Show References
Clinical Question:
- Does dexmedetomidine lead to better short-term and long-term outcomes than propofol in mechanically ventilated adults with sepsis?
Methods:
- Multicenter (13 US hospitals), double-blinded, 422 mechanically ventilated patients with sepsis
- Notable exclusion criteria: pregnant, 2nd- or 3rd-degree heart block or persistent bradycardia requiring intervention, indication for bzds, expected to have NMB > 48 hrs, already had received mechanical ventilation >96 hrs
- Pain was treated with opioid pushes or fentanyl gtt
- Primary end point: number of calendar days alive without delirium or coma during the 14-day intervention period
- Secondary efficacy end points included ventilator-free days at 28 days, death at 90 days, and global cognition at 6 months
Results:
- No sig difference in adjusted number of days alive without delirium or coma over the 14-day intervention period (dexmedetomidine: 10.7 days vs. propofol: 10.8 days; OR, 0.96; 95% CI, 0.74 to 1.26; P = 0.79
- No sig differences in the number of ventilator-free days at 28 days, in death at 90 days, or global cognitiion at 6 months
- Other notable findings:
- Fewer patients in the dexmedetomidine group had ARDS or signs of trial drug withdrawal
- Fewer patients in the propofol group extubated themselves
- Open-label propofol received by 13% in the dexmedetomidine group and 8% in the propofol group) and dexmedetomidine (4% in the dexmedetomidine group and 3% in the propofol group)
- Rescue midazolam was used in about half the patients, most often for procedural sedation or during NMB, 42% received antipsychotics
- Similar proportions of patients had organ dysfunction, hypotension, or severe lactic acidosis
- Symptomatic bradycardia requiring discontinuation of the trial drug was similar in the two groups
Take-home points:
- Dexmedetomidine or propofol are reasonable options for septic patients requiring mechanical ventilation without notable differences in delirium or mortality
Show References
Background: In respiratory failure due to COPD and cardiogenic pulmonary edema, noninvasive positive pressure ventilation decreases need for intubation and improves mortality,1 while its utility in other scenarios such as ARDS and pneumonia has yet to be proven.1,2 We know that patients on NIV with delays to needed intubation have a higher mortality,1,3 but intubation and mechanical ventilation come with risks that it is preferable to avoid if possible.
So how and when can we determine that NIV is not working?
The HACOR (Heart rate, Acidosis, Consciousness, Oxygenation, Respiratory rate) score at 1 hour after NIV initiation has been demonstrated to be highly predictive of NIV failure requiring intubation.4,5
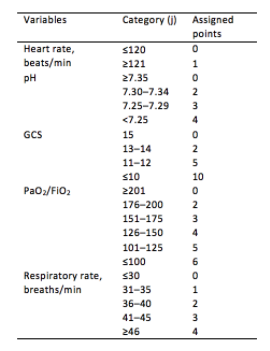
Initial development/validation: Score > 5 after 1 hour of NIV corresponds to >80% risk of NIV failure4
-
Earlier intubation (before 12 hours) in these patients = better survival
External validation: Score > 8 after 1 hour of NIV most predictive of eventual NIV failure 5
-
Average score @ 1-hour of patients with NIV success = 3.8
-
Score remained predictive at 6, 12, 24, 48 hours as well & mortality worsened as delay to intubation time increased
-
Baseline, pre-NIV score not predictive
-
Better predictive agreement in pneumonia and ARDS
Bottom Line:
-
Patients on NIV require close reassessment to prevent worsened survival due to intubation delay should invasive mechanical ventilation be indicated.
-
A HACOR score >8 after 1 hour of NIV should prompt intubation in most instances, with strong consideration given to a score >5.
*Note: ABGs were obtained for PaO2 assessment in the above studies -- the use of SpO2 was not evaluated -- but we are often not obtaining ABGs in our ED patients with acute respiratory failure. The following chart provides an estimated SpO2 to PaO2 conversion.
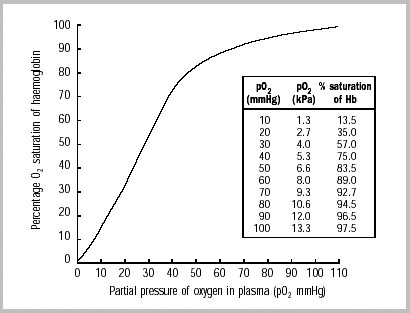
WHO 2001
Caveats:
- Pulse oximetry may be inaccurate in darker skin tones (overestimated by ~2%)6 and in certain disease processes (e.g. CO poisoning, profound shock states, etc.)
- The oxyhemoglobin dissociation curve shifts right with increasing pCO2/decreasing pH (lower saturation for a given PaO2).
Show References
Optimal oxygenation targets and the possible, theoretical, benefits of hyperoxygenating critically ill patients have long been points of controversy. Multiple studies have suggested harm in pursuing aggressive hyperoxygenation amongst critical patients with various conditions ranging from myocardial infarction to sepsis to neurologic conditions. In addition, oxygen toxicity is a known mechanism causing ARDS.
The HOT-ICU trial adds to the list of arguments against hyperoxygenation, by looking at 2928 ICU patients on high levels of supplemental oxygen and targeting a paO2 of 60 mm Hg (low oxygen group) vs paO2 of 90 mm Hg (high oxygen group). There was no difference in mortality, or other significant difference in outcomes.
Bottom Line: A lower paO2 goal of 60 (correlates to an O2 sat of 90%) is noninferior to a higher paO2 goal of 90 (O2 sat of approximately 96%). When titrating oxygen, targeting a pulse ox of 90-96% is reasonable in critically ill patients. Be sure to include an upper limit on the sat goal, beware an O2 sat of 100%, and titrate down supplemental oxygen when the spO2 is above goal, as the paO2 may be dangerously high.
Show References
Mechanical Ventilation in COPD
- Mechanical ventilation of the patient with obstructive lung disease can be challenging, primarily due to the presence of dynamic hyperinflation.
- In the initial phase of ventilation, it is important to prevent complications of hyperinflation and not to target normalization of blood gas values.
- Recommended initial ventilator settings include:
- Mode: Volume assist-control
- Inspiratory flow waveform: square
- Tidal volume: 6-8 ml/kg PBW
- RR: 12 bpm
- Inspiratory flow: 60-90 L/min
- The effect of PEEP is variable with each patient. When titrating PEEP, be sure to frequently measure plateau pressure and discontinue titration should Pplat increase.
Show References
| Ever wonder what to tell the families regarding prognosis of the sickest COVID-19 patients you intubate in the ED or ICU? Introduction: Case fatality rates (CFR) for COVID-19 patients requiring invasive mechanical ventilation have been widely variable. A study in the Blue Journal (AJRCCM) examined patients requiring intubation in a systemic review and meta-analysis. The case fatality risk of an infection is represented by the proportion of patients who die among all infected cases in a population over a period of time. Methods: 69 studies axross 23 countries for a total of 57,420 patients with COVID-19 who required mechanical ventilation were included in analysis. Results: Overall case fatality rate was 45%, or about 1 death for every two intubated patients.. Among studies that included age stratification, pooled estimates of CFR were 47.9% in patients <40 (CI 46.4-49.4%) and 84.4% in patients >80 (CI 83.3-85.4%). Overall heterogeneity is high (I 2 .90%), In early COVID epicenters, CFR was 70% among patients aged more than 60 years of age. CFR increased exponentially with increasing age. Specifically in the US across 21 studies (3,811 intubated patients), CFR was 47% (95% CI, 36–57%). Studies from New York reported a CFR of 54% (95% CI, 36–72%) whereas other regions in the United States reported a CFR of 41% (95% CI, 30–53%). Definitive hospital CFR (aka for those with hospital discharge outcomes, 13,120 patients) was 56% (CI 47-65%). Conclusion: Almost half of patients with COVID-19 receiving IMV died based on the reported CFR. The reported CFR was higher in older patients and in early pandemic epicenters, which may be influenced by limited ICU resources. Limitations: Overall CFR of 45% still included patients in the hospital. Definitive hospital outcomes were only for 13,120 patients (36.6%). Significant variation in CFR exists between studies. |
Show References
A single center (Nebraska, USA), retrospective analysis investigated the prevalence of intubation during hospital stay for 105 patients who had COVID-19 between March 24 to May 5, 2020 (1). 40 patients underwent awake proning vs. 60 patients did not undergo awake proning.
After adjusting for either SOFA or APACHE scores, patients with awake proning were associated with lower Hazard Ratios of intubation for SOFA (HR 0.30, 95% CI 0.09-0.96, p=0.043) and APACHE (HR 0.30, 95%CI 0.1-0.91, p=0.034).
Discussion
While this US study seemed promising, another Brazilian study being published earlier in July 2020 showed no difference in the prevalence of intubation between COVID-19 patients with proning or without proning (2).
These 2 studies highlighted the nature of this disease: high practice variability, uncertainty of therapeutic modalities. However, the complications from awake proning had been very low.
Conclusion:
Awake proning for hypoxic COVID-19 patients is a promising intervention but we will need more studies. In the meanwhile, we can try this therapeutic modality as the risk is low.
Show References
Study Question: What is the association of relative hypotension (degree and duration of MPP deficit) in patients with vasopressor-dependent shock with the incidence of new significant AKI and major adverse kidney events (MAKE)?
- Mean Perfusion Pressure (MPP) = MAP - CVP
- MAKE-14: composite measure of death, new initiation of RRT, or doubling of serum creatinine from the premorbid level at Day 14
- Basal MPP estimated using pre-illness BP readings in the chart, basal CVP estimated using prior echo findings or estimated mean values
Methods:
- Multicenter, prospective observational cohort study with 302 patients
- Notable exclusion criteria:
- age < 40, trauma as primary reason for ICU admission, active bleeding, unavailability of at least two preillness BP readings, pregnancy, "any condition specifically requiring a higher or a lower blood pressure target in the view of a treating clinician"
Results:
- for every percentage increase in the time-weighted average MPP deficit, the odds of developing new significant AKI and MAKE-14 increased by 5.6% (95% CI, 2.2–9.1; P = 0.001) and 5.9% (95% CI, 2.2–9.8; P = 0.002), respectively.
- Relationships between the risks of developing new significant AKI or MAKE-14 and the percentage of time spent with a MAP < 65 mm Hg were not statistically significant
Take-aways:
- Critically ill patients in shock who had higher and longer degrees of relative hypotension compared to their baseline BPs had a higher incidence of adverse kidney outcomes
- Sidenote: also consider venous congestion/volume overload when thinking about end-organ damage (e.g. MPP not just MAP)
Show References
PEEP in the Intubated Obese Patient
- Obesity has numerous adverse effects on the respiratory system, most notably a reduction in lung volumes.
- The reduction in lung volumes (i.e., FRC) often result in airway closure and atelectasis.
- The application of PEEP in the mechanically ventilated patient helps maintain alveolar patency by preventing derecruitment.
- Importantly, the typical initial PEEP setting of 5 cm H2O is insufficient for many ventilated obese patients.
- Pearl: In the ventilated obese patient start with an initial PEEP of 10-15 cm H2O.
Show References
Summary
Our group performed a meta-analysis to assess whether it is safe to infuse vasopressor through peripheral venous catheters. We identified 9 studies with a total of 1835 patients. The prevalence of complications among the pooled patient population was 9%. Up to 96% of the complications was extravasation and almost no complications required any treatment.
A few studies reported safe infusion of norepinephrine up to 0.1 mcg/kg/min for up to 24 hours.
In exploratory meta-regression, catheter size 20 or larger was negatively associated with the rate of complications.
We also observed that studies that were published within the past 5 years reported significantly lower rate of complications from older studies. This suggested that with careful planning and monitoring, it is safe to start vasopressor through peripheral IV.
Limitation
most of the included studies were observational. No studies had enough power to statistically analyze any variables that could predict complications.
Bottom line: we should start vasopressor as soon as indicated, if we have good, reliable IV access.