Search
Warfarin-Induced Skin Necrosis (WISN)
Some pearls about a rare, but serious side effect of Warfarin...
- WISN Occurs in 0.01-0.1% of patients taking Warfarin
- More common in middle-age, perimenopausal women being treated for DVT/PE
- Symptoms usually begin on days 3-6 of Warfarin treatment
- Underlying pathophysiology is complex but involves thrombosis of superficial dermal capillaries
- Postulated to be associated with deficiencies of protein C, protein S, and antithrombin III
- Rash is most common on the breats, with thighs/buttocks being second most common site (see picture)
- Diagnosis usually made clinically based on appearance of rash
- Treatment is aimed at restoring Vitamin K dependent clotting factors by administering Vit K and FFP
- For patients with the need for anticoagulation (DVT/PE, etc.) Heparin therapy is usually started

55 yo female presented to the ED on the day of hospital discharge for evaluation of this rash.
The rash began 4 days after starting Warfarin. Was being treated for a DVT.
Attachments
SIDS
Sudden infant death syndrome (SIDS) is defined as the sudden death of an infant younger than 1 year that remains unexplained after a thorough case investigation, including the performance of a complete autopsy, examination of the scene of death, and review of the clinical history.
SIDS is the single most common cause of death in infants aged 1 mo to 1 yr
Education is key for prevention of these tragic events:
Following the "Back to Sleep" campaign, federal SIDS researchers have conducted annual surveys to examine how infant sleep practices and SIDS rates have changed. The rate of prone sleeping for infants decreased from approximately 75% in 1992 to a low of 11.3% in 2002
Since 1992, SIDS rates have fallen approximately 58%. In 2002, the National Center for Health Statistics reported a total of 2295 SIDS deaths nationwide for a SIDS rate in the United States of 0.51 per 1000 live births.
Bed-sharing may lead to compromise of the infants' airway because the infant may be suffocated by soft, loose bedding or a sleeping adult.
Cosleeping on a couch or sofa is associated with an unusually high risk for SIDS and should be avoided.
Tryptophan - a precursor to melatonin, it is often blamed for the post prandial coma that many go into after a big turkey dinner. Never mind the 5000 kcals that was consumed during the meal. The supplement really doesn't help with sleeping. Interestingly, turkey isn't even in the top 10 or 20 of foods that contain tryptophan. The top five are:
1) Game meat (Elk): 746 mg of tryptophan
2) Seaweed (Spirulina): 736 mg of tryptophan
3) Spinach: 690 mg of tryptophan
4) Egg White: 673 mg of tryptophan
5) Soy protein: 630 mg of tryptophan
Supplements of L-tryptophan have been contaminated with a compound that has been associated with eosinophilia myalgia syndrome.
Stress Related Mucosal Injury (SRMI)
- As the length of stay for many of our critically ill patients continues to rise, it is important to think about some preventative therapies
- SRMI is the term used to describe gastric mucosal erosions that occur in the critically ill
- SRMI can be demonstrated in 75 - 100% of critically ill patients within 24 hours and can cause clinically apparent bleeding in up to 25%
- Independent risk factors for SRMI include mechanical ventilation, coagulopathy, and a prior history of gastritis or peptic ulcer disease
- Additional risk factors in our ED patient population include sepsis, hypotensive states, severe head injury, multisystem trauma, and renal failure
- Typically an H2 antagonist is provided (i.e. ranitidine or famotidine). Currently there is no evidence of superiority of PPIs over H2 antagonists in preventing SRMI
- Pearl: the best agent to give is probably sucralfate - there is a slightly higher incidence of bleeding compared to ranitidine; however, ranitidine is associated with a much higher incidence of nosocomial pneumonia. The risk and mortality associated with nosocomial pneumonia in these patients outweighs the minimal risk of major hemorrhage associated with SRMI
What Hypertensive Patient Needs a Workup for End-Organ Damage?
Ah, the age old question...which hypertensive patients need an ED workup for end-organ damage? The "workup" for patients includes renal function, urinalysis, CXR, ECG, etc.
Some pearls regarding working patients up:
- Asymptomatic patients in general do not need a workup. There is pretty good literature that shows you just won't find much (expecially anything that will change your treatment plan) if you go hunting in this group of patients.
- If you set asymptomatic patients aside, you won't find much good data on how much of a workup other patients need. Does a 45 yo patient with a BP of 160/110 and a mild HA need a serum creatinine? What if they have had some mild, atypical CP? The answer is...no one knows. Much of what we we do depends on what we were taught and our current mood.
- Asymptomatic patients (truly asymptomatic) don't need chest xrays and ECGs as a rule of thumb...what you find won't help you make a decision. If you find LVH on the ECG, so what?
- Obtaining a serum creatinine makes sense, especially of you are going to start a BP agent.
- There is a pretty good study by Karas, et al. that showed that a urinalysis without protein or blood predicts a normal creatinine. Use caution, however, if you use this as a screen for renal disease, because many patients with HTN spill protein (despite a normal creatinine)
Third Trimester Bleeding:
- Estimated to occur in 4% of Pregnancy
- 50% will have a benign cause, the other 50% will have a life threatening cause
- Life Threatening Causes:
- Benign or Non-OB Causes
- Contact Bleeding (local trauma)
- Cervical Inflammation (i.e. infection)
- Cervical effacement and dilation
- Cervical cancer
- Other sites:
- rectal bleeding
- urinary bleeding
- Evaluation:
- ABC's: Stablilize mother, consider 2 large bore IVs
- Consult OB/GYN early (most centers with OB/Gyn will have these patients evaluate and treated in Labor and Delivery), if not readily available complete evaluation as listed below:
- Initially avoid bimanual exam
- Obtain baseline labs (CBC, Coags, Chemistries, Consider LFTs if suspecting eclampsia or HELLP syndromes). If not known obtain Rh status
- Fetal Monitioring ideally with continous fetal heart rate and tocometry
- Sterile Speculum exam for culture and check for active bleeding.
- Obtain ultrasound.
- Phenytoin (Dilantin) should not be infused at a rate greater than 50 mg/minute, to a total of 20 mg/kg.
- Caution is encouraged while infusing due to the risk of inducing hypotension and cardiac arrhythmias, making cardiac monitoring during infusion mandatory.
- These adverse effects are partly related to the propylene glycol used to solubilize phenytoin.
- Additionally, the risk of local pain and injury, such as venous thrombosis and the purple glove syndrome, increases with rapid infusion rates.
Dopamine in the ED
- Recall that dopamine is an endogenous catecholamine that is a precursor for norepinephrine synthesis
- Despite the popularity of norepinephrine, dopamine is still used by many EPs in the setting of septic shock
- Dopamine produces progressive alpha-receptor stimulation at doses > 10 mcg/kg/min
- Tachyarrhythmias (namely sinus tachycardia) is the predominant adverse effect
- When selecting a vasopressor agent, be sure to check the HR. If the patient is already tachycardic, the addition of dopamine will only worsen the tachycardia
- Additional important adverse effects are increased intraocular pressure and delayed gastric emptying
Show References
Healthcare Associated Pneumonia (HCAP)....why is this important for the emergency physician?
Most of us are very familiar with the types of pneumonias commonly seen in clinical practice: community-acquired pneumonia (CAP), hospital-acquired pneumonia(HAP), and ventilator-associated pneumonia (VAP). But, some may not be that aware of a relatively newer type of pneumonia that has been well-defined, healthcare-associated pnemonia (HCAP). Experts in infectious disease and critical care now say that we (the ED) should be assessing ALL pneumonia patients for HCAP risk factors.
Why care, you ask?
- Higher mortality than CAP
- May look like CAP
- Treated much differently than CAP
Risk factors: (most are common sense)
- Nursing home or extended care facility resident
- Recently admiited to a hospital for 2 or more days in the preceeding 90 days
- Home wound care or attending a clinic for wound care
- Dialysis patient
- Home infusion therapy (antibiotics)
- Immunosuppresive therapy or disease
Treatment:
- 3 drugs....not like treatment of CAP!
- Usually a combination of a big gun anti-pseudomonal (e.g. Pip/Tazo) combined with a broad spectrum respiratory fluoroquinolone (e.g. Moxi), combined with Vancomycin
- Key difference between treatment of CAP and HCAP is consideration for multi-drug resistant pathogens, pseudomonas, and MRSA.
Death from ruptured aortic aneurysms and thoracic aortic dissection has a few key features that often help in distinguishing these entities from other causes of rapid decompensation and sudden death:
1. These aortic disasters have a tendency to present with hypotension but without necessarily any specific complaints of pain (in contrast to common teaching).
2. These aortic disasters tend usually to produce PEA as the initial arrest rhythm.
3. These aortic disasters are often diagnosable on bedside ultrasound (AAA seen when scanning the abdomen; dissections frequently produce pericardial tamponade as they dissect backwards into the pericardial sack).
ALWAYS take a look at a patient's aorta and pericardium with the ultrasound when that patient presents in extremis or in cardiac arrest. The results can help make some critical diagnostic and therapeutic decisions.
[recent article related to this topic: Pierce LC, Courtney DM. Clinical characteristics of aortic aneurysm and dissection as a cause of sudden death in outpatients. Am J Emerg Med 2008;26:1042-1046.]
The glucometer is one of the devices that we quickly reach for in the management of our unresponsive patients, diabetics and in the critically ill. Recently, I noticed that our Roche Accu-Check has a big sticker on the case stating that results could be affected by therapies that alter the metabolism of galactose, maltose, and xylose. Since this was a big hole in my fund of knowledge I decided to look up what else affects the accuracy of glucometers.
Now, Dr. Winters already warned used about the inaccuracy of bedside glucometer readings in the critically ill, but what about the patient that is not septic and/or in shock.
Substances/Drugs that have been reported to affect the accuracy of glucometers are:
- Levodopa
- Dopamine
- Mannitol
- Acetaminophen
- Severe lipemia
- Severe unconguted bilirubin
- Elevated Uric Acid
- Maltose (present in immunoglobin products)
- Patient on peritoneal dialysis secondary to Icodextrin
- Ascorbic Acid (Vitamin C)
Anemia also results in higher values, and a capillary blood sample can differ from venous blood by as much as 70mg/dL.
Most errors are more significant when dealing with hypoglycemia.
So the moral of the story is be careful with a bedside glucometer when the reading is low, as the venous blood sample sent to the lab may return even lower. Error on the side of treating the patient with glucose.
Show References
- Exact definitions of status epilepticus vary.
- Generally speaking, status epilepticus is defined as a single unremitting seizure that lasts longer than 5 to 10 minutes OR greater than one generalized clinical seizure with no interictal return to clinical baseline.
- While treatment with phenytoin and diazepam is often used for status, studies have shown that lorazepam use alone is more effective.
How many times have you had a patient with an allergy to codeine described as stomach upset? Or how about a rash with morphine (probably secondary to histamine release)? True anaphylactic reactions to opioids are very rare (< 1%). But what happens when you have a patient with a true allergy, but still need to give an opioid? No problem, you just need to choose one that is structurally different.
- Group 1 (aka opiates) - Naturally occurring agents derived from the opium plant
- Morphine, codeine, thebaine
- Group 2 - Semi-synthetics
- Hydrocodone, oxycodone, hydromorphone, oxymorphone, buprenorphine (heroin is also in this group)
- Group 3 - Synthetics
- Fentanyl (alfentanil, sufentanil, etc.), methadone, tramadol, propoxyphene, meperidine
All of the group 1 and 2 agents are structurally very similar to each other and should not be given if a true allergy exists to any other natural or semi-synthetic derivative. Group 3 agents have structures different enough that they can be given to a patient intolerant to the natural or semi-synthetics without fear of cross reactivity. They are also very different from others in this same group.
Seizures in the Critically Ill
- Seizures are a common complication in medical and surgical patients commonly arising from coexisting conditions associated with critical illness
- Most seizures in the critically ill are generalized convulsions rather than focal
- The majority of seizures occur in patients without a pre-existing history of seizure disorder
- Common causes of seizures in the critically ill include sepsis, cardiovascular disease, metabolic abnormalities, medications, and drug intoxication/withdrawal
- Metabolic abnormalities account for 30 -35% of causes
- The most common metabolic abnormalities include hyponatremia, hypocalcemia, hypophosphatemia, uremia, and hypoglycemia
- Be sure to check these labs in ICU patients with a seizure
Show References
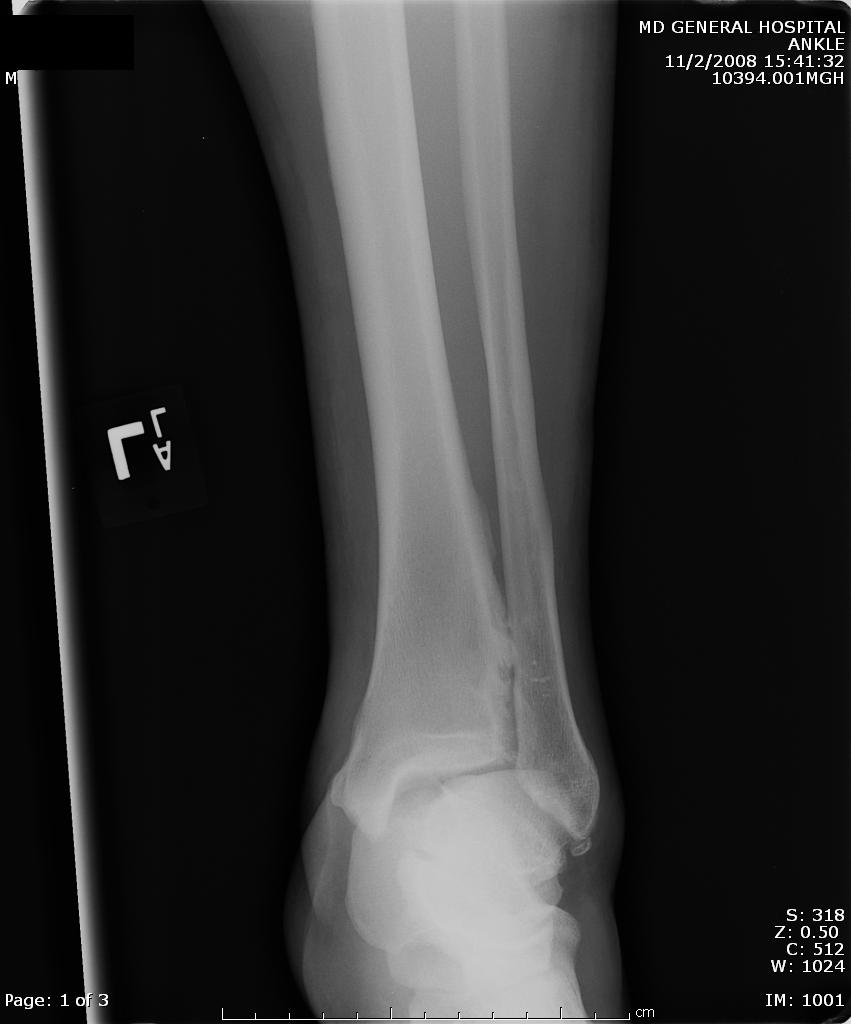
A maisonneuve fracture is a fracture dislocation resulting from external rotational forces to ankle -- through interosseous ligament to fibula.
- Proximal fibula fracture - from external rotational forces (spiral/oblique)
- Ankle components can include any of the following:
- medial maleolus avulsion fx or deltoid ligament rupture
- anterior talofibular ligament rupture
- interosseous ligament rupture
- posterior malleolar fracture
If stability is questionable, orthopedic evaluation under anesthesia is required. Additionally always consider compartment syndrome. Do not rely on Kanduval's signs (pain, paraesthesia, pallor, poikilothermia, pulselessness) - "... with the exception of pain and paraesthesia, these traditional signs are not reliable." Emergent orthopedic consultation and compartment pressure assessment should be performed. (see attached photos)