Search
1-13 of 13 results by Dan Lemkin
Many physicians have the opportunity to invest in a variety of retirement funds. The most common commercial vehicle is a 401k. Academic and non-profits have access to an analogous 403b. Many physicians also have access to a 457b.
It is important to understand what it is, and most importantly how it differs from a conventional 401k or 403b. Like its' peers, it permit pre-tax contributions of a finite amount. They are offered through your employer and are bound to a specific vendor(s). These vendors provide a select number of investment choices specific to the employer contract. The maximum contribution for 2012 is $17,000.
The 457b is different from the other investment vehicles because of who and where your funds are held:
Non-governmental 457 plans have a number of restrictions that governmental ones do not. Money deferred into non-governmental 457 plans may not be rolled into any other type of tax-deferred retirement plan. It may be rolled only into another non-governmental 457 plan. Also, money deferred into non-governmental plans is not set aside in a trust for the exclusive benefit of the employee making the deferral. The Internal Revenue Code requires that money in a non-governmental 457 plan remains the property of the employer and is thus available to general creditors of the employer in legal or bankruptcy
If you work for a private entity, or a non-profit and they offer a non-governmental 457b, your personal funds are pooled with corporate resources. Your retirement contributions are at risk, should the company default and declare bankruptcy. This risk is apparently not born by GSRA 457b (Governmental agency 457b plans). A decade ago, this risk would seem insignificant. With the number of large companies and municipalities defaulting in this economic climate, prudence is warranted when considering this investment vehicle. DISCLAIMER - This pearl is not intended to provide financial advice. Please consult your HR department and / or financial advisor for additional information and advice.
![]()
Dear Readers,
Thank you for your continued interest in the University of Maryland's EM Pearls program. We are conducting a survey to assess whether our pearls are meeting your needs. Data collected will be used to refine and improve our educational program. Please take 1 minute to complete our survey by clicking the link below.
http://umem.org/surveyor/index.php?sid=86815&newtest=Y&lang=en
If you regularly forward pearls to other readers, please forward this message as well. We wish to capture as many readers' opinions as possible.
If you have any questions or problems, please contact: admin@umem.org
Sincerely,
Dan Lemkin, MD MS
EM Pearls Development Team
University of Maryland School of Medicine
Department of Emergency Medicine
Chlorhexidine (CHG) has rapidly become the antiseptic of choice for most skin preparation prior to any percutaneous procedures including:
- venipuncture
- laceration repair,
- joint aspiration
- lumbar puncture???
The Chlorprep(R) label notes: "DO NOT USE FOR LUMBAR PUNCTURE OR IN CONTACT WITH THE MENINGES" (attached)
Authors of the British Royal College of Anaesthetists 3rd National Audit Project provided some guidance for the use of chlorhexidine for spinal procedures
- Clinicians must take care to prevent CHG from reaching the CSF
- Keep CHG away from other drugs and equipment being used
- Allow solution to dry prior to beginning procedure
- Avoid using solutions > 0.5% chlorhexidine
- Further comments
- Chlorhexidine 0.5% in alcohol 70% is the optimal skin preparation for neuroaxial procedures
- Risk of vertebral canal sepsis is greater than the very rare risk of neurotoxicity and arachnoidits from chlorhexidine
- This is OFF-LABEL use and should be instituted formally at a departmental level with an audit process for complications
Further: Correspondance from the Journal of Regional Anesthesia and Pain Medicine
"Dr. David Hepner published a correspondence in the April 2007 issue of Anesthesiology that stated the expert panel for Regional Anesthesia and Pain Medicine “felt strongly that although the US Food and Drug Administration has not approved chlorhexidine before lumbar puncture, it has a significant advantage over povidone iodine because of its onset, efficacy, and potency” and commented that “interestingly, povidone iodine is also not approved for lumbar puncture."
Chlorhexidine off-label use is supported in academic literature. Due to specific labeling prohibiting use, a formal institutional policy to support such use may be indicated.
Show References
Attachments
Hydrofluoric acid is a weak acid used primarily in industrial applications for glass etching and metal cleaning/plating. It is contained in home rust removers. Although technically a weak acid, it is very dangerous and burns can be subtle in appearance while having severe consequences.

Wilkes G. Hydrofluoric Acid Burns. Jan 28, 2010.
http://emedicine.medscape.com/article/773304-overview
- 2 mechanisms that cause tissue damage*
- corrosive burn from the free hydrogen ions
- chemical burn from tissue penetration of the fluoride ions
- Clinical features*
- Cutaneous burns - absent findings to white-blue appearance
- Pulmonary edema
- Hypocalcemia, hyperkalemia, hypomagnesemia
- Treatment*
- Decontaminate by irrigation with copious amounts of water.
- With any evidence of hypocalcemia, immediately administer 10% calcium gluconate IV.
- Cutaneous burns:
- Apply 2.5% calcium gluconate gel to the affected area. If the proprietary gel is not available, constitute by dissolving 10% calcium gluconate solution in 3 times the volume of a water-soluble lubricant (eg, KY gel). For burns to the fingers, retain gel in a latex glove.
- If pain persists for more than 30 minutes after application of calcium gluconate gel, further treatment is required. Subcutaneous infiltration of calcium gluconate is recommended at a dose of 0.5 mL of a 5% solution per square centimeter of surface burn extending 0.5 cm beyond the margin of involved tissue (10% calcium gluconate solution can be irritating to the tissue).
- Do not use the chloride salt because it is an irritant and may cause tissue damage.
*Extracted from emedicine article.
Show References
Winged scapula is caused by muscular injury or damage to corresponding muscular innervation. Mechanism can be due to blunt or penetating thoracic trauma.
- Trapezius muscle
- Long thoracic nerve
- Serratus Anterior muscle
- Spinal Accessory Nerve
Clinical findings include
- Protruding medial edge of the scapula
- Exacerbation by pushing against resistance
- Difficulty lifting arm over head
Treatments
- Initial splinting and orthopedic referral
- Depending on mechanism - trial of physical therapy
- Surgical treatments include fascial grafts or adjacent muscle attachment

Show References
Beware of your online contributions, they can come back to hurt you in legal settings. You must remember that there is a digital trail of everything you post online. Discovery rules vary state to state. It is best to practice save surfing. What you may perceive as paranoia is really just good practice.
The following guidelines apply to:
- Online chats: google chat, IRC, AOL AIM, MSN
- Social networks: Facebook, Mypage, Medical networking pages, etc
- Any online medium, forum, discussion site
General guidelines
- Do not reference any patient cases with dates (regardless of hipaa identifiers)
- Do not provide any medical advice for specific cases online
- Add a disclaimer for general advice (see the disclaimers for these pearls as example)
- Do not discuss any potential or ongoing legal cases with peers PERIOD, especially electronic methods with a record.
- Do not document ethically questionable behavior online
- ie: "that time in vegas when you got sooooo drunk"
Assume that whenever you hit send, your message will be available to a plaintiff attorney who will twist it to suit his/her needs. The only potential exception is direct email communication to your personal legal counsel. Please verify that local laws protect this form of communication before making an assumption of privacy.
[This pearl is a review of published general recommendations on privacy practices and should not be interpreted as, or replace competent legal advice.]
Show References
Jones fracture
- Fracture of proximal metaphyseal 5th metatarsal
- located w/in 1.5 cm distal to tuberosity of 5th metatarsal
- Prone to malunion
- Watershed area (poor blood supply)
- Under tension from multiple tendons
- Treatment
- Immobilize with posterior-mold splint
- Non-weight bearing - crutches
- Prompt orthopedic evaluation
- Some cases are managed with non-weight bearing casts
- Others are repaired operatively.
- Delayed jones fractures with malunion will require operative repair.
- Distinguish from pseudo-jones fracture (dancers fracture)
- metatarsal styloid avulsion fracture, generally does not require operative repair
- much more common than true Jones fracture.
Presented with persistant foot pain from
Jones fracture malunion.

Show References
Classical illicit recreational drugs like cocaine, ecstacy, and marajuana are sometimes difficult for teens to acquire. As a result, many are turning to their parents medicine cabinets as a source for recreational drugs.
[From the website drugabuse.gov] In 2008, 15.4 percent of 12th-graders reported using a prescription drug nonmedically within the past year. This category includes:
- amphetamines
- sedatives/barbiturates
- tranquilizers
- opiates other than heroin
- hydrocodone, oxycodone
When adolescent patient presents to the ED, consider the possibility of a poly-pharmacy overdose. Always query parents about the presence of OTC and Rx medications in their home, and what is within reach of their kids.
While sedatives and analgesics are concerning, be alert for overdoses of more mundane medications like beta blockers and calcium-channel blockers which often pose a much more lethal threat. Consider overdose in adolescent patients with:
- GI or respiratory complaints
- Altered mental status (combative or somnolent)
- Abnormal vital signs
- History of depression or psychiatric illness
Monitoring the Future Study: Trends in Prevalence of Various Drugs for 8th-Graders, 10th-Graders, and 12th-Graders
2005-2008 (in percent)*
| 8th-Graders | 10th-Graders | 12th-Graders | ||||||||||
| 2005 | 2006 | 2007 | 2008 | 2005 | 2006 | 2007 | 2008 | 2005 | 2006 | 2007 | 2008 | |
| Any Illicit Drug Use | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lifetime | 21.4 | 20.9 | [19.0] | 19.6 | 38.2 | 36.1 | 35.6 | 34.1 | 50.4 | 48.2 | 46.8 | 47.4 |
Full chart available by clicking link in references.
Show References
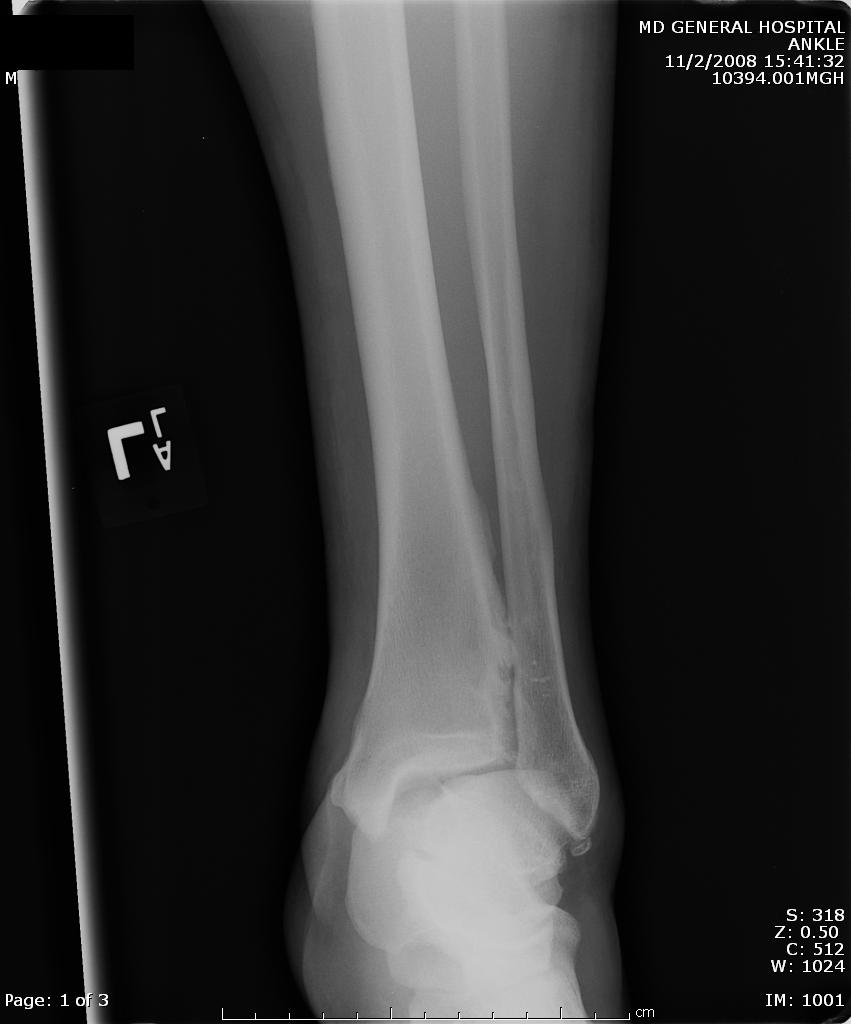
A maisonneuve fracture is a fracture dislocation resulting from external rotational forces to ankle -- through interosseous ligament to fibula.
- Proximal fibula fracture - from external rotational forces (spiral/oblique)
- Ankle components can include any of the following:
- medial maleolus avulsion fx or deltoid ligament rupture
- anterior talofibular ligament rupture
- interosseous ligament rupture
- posterior malleolar fracture
If stability is questionable, orthopedic evaluation under anesthesia is required. Additionally always consider compartment syndrome. Do not rely on Kanduval's signs (pain, paraesthesia, pallor, poikilothermia, pulselessness) - "... with the exception of pain and paraesthesia, these traditional signs are not reliable." Emergent orthopedic consultation and compartment pressure assessment should be performed. (see attached photos)




Show References
Abdominal pain can be very confusing. Occasionally, serious etiologies may masquarade as benign complaints. Always consider the following pitfalls when addressing abdominal complaints.
- Be aware of extra-abdominal disease processes presenting as abdominal pain
- AMI, pneumonia, pelvic diesases
- If you suspect appendicitis - than pursue the diagnosis
- Do not delay notification of surgeon, and request consultation early
- It is reasonable for them to examine the patient without CT results
- It is not reasonable to withhold pain medications until they see the patient
- Time all calls, and document all discussions with consultant name
- Do not delay notification of surgeon, and request consultation early
- UTI and gastroenteritis should be considered diagnoses of exclusion. Be wary of using, if any red flags exist
- fever, hypotension, blood in stool, weight loss, abdominal tenderness
- Unless the diagnosis/etiology is clearly not pelvic in origin, always do a pelvic exam in a women
- Always consider, and document your consideration of testicular and ovarian torsion
- In a septic patient with UTI, consider obstructing pyelonephritis.
- Patients with a kidney stone and obstructing pyelo will not get better unless the stone is removed. CT for stones, prior to dispo.
- Consider vascular etiologies in high risk populations: elderly, diabetic, hypertensive
- AAA - pain to back, tearing sensation
- Dissection - pain, decreased pulses, neuro findings
- Mesenteric Ischemia / schemic Colitis - pain out of proportion to exam findings
- Torsion - radiating pain to abdomen - document a genital exam
Disclaimer: This information does not constitute legal advice, is general in nature, and because individual circumstances differ it should not be interpreted as legal advice. The speaker provides this information only for Continuing Medical Education purposes.
Content abstracted from: Nguyen Anh, Nguyen Dung. Learning from Medical Errors. Radcliffe Publishing, UK. 2005. P 11-13.
A recent study came out which confirms what we already knew... that MRSA infections are no longer confined to ICUs but are spreading to the community. What the new study does show, is that it affects particular populations disproportionately and Baltimore City, more than any other study population. The full article is attached below, or can be obtained for free from the JAMA website.
| "Unadjusted incidence rates of all types of invasive MRSA ranged between approximately 20 to 50 per 100 000 in most ABCs sites but were noticeably higher in 1 site (site 7, Baltimore City) (TABLE 2)." "... we calculated interval estimates excluding site 7 (Baltimore City) to allow the reader to interpret a range of estimates reflecting different metropolitan areas. Regarding the high observed incidence rates reported by site 7, we conducted an evaluation to determine whether these results were valid, including a review of casefinding methods, elimination of cases to include only those with zip codes represented in the denominator, contamination in any laboratory, and other potential causes for increased rates; however, none were in error." |
Attachments
Why do you care?
Well, many email clients will block html, or messages that have lots of capitals, decorations, etc...
Our first priority is to get you the information and beat anti-spam auto-filtering. If you notice that you are not getting the educational emails.
- Add admin@umem.org and umem.org to your safe senders list
| Notes to authors
|
dan