Search
Background: Prior evidence1,2 has suggested that early “pan-scan” after ROSC provides clinically-relevant information that assists in the care of the patient in question, when the cause of OHCA is unclear.
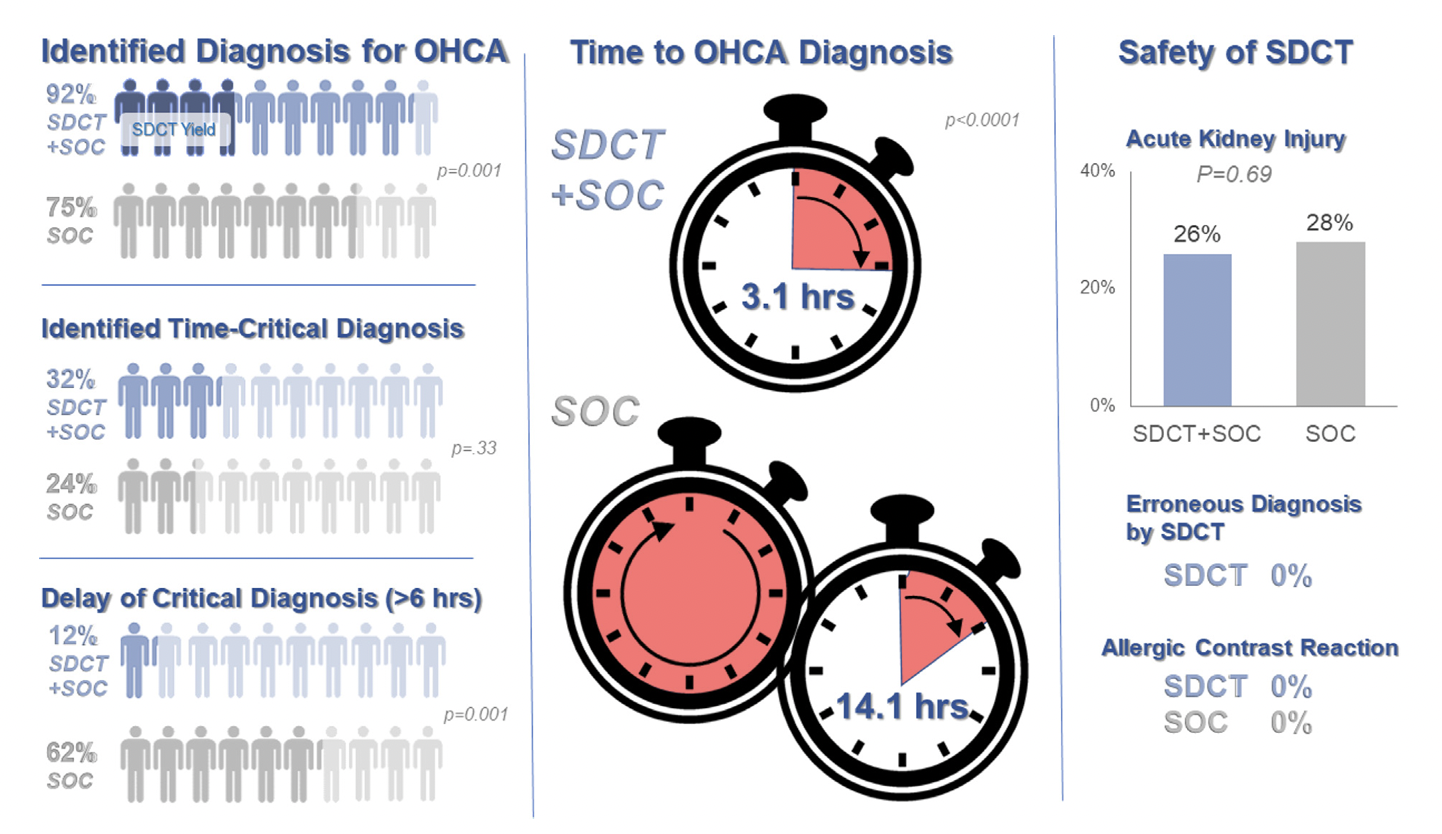
The recent CT FIRST trial looked at patients pre- and post- implementation of a protocol for head-to-pelvis CT within 6 hours of ROSC for adult patients without known cause or evidence of possible cardiac etiology, stable enough for scan. *Patients with GFR <30 were excluded from assignment to CT, although were included in the post/CT cohort if their treating doctors ordered CT scans based on perceived clinical need. To balance this, a similar number of patients with GFR <30 were included in the pre/“standard of care” cohort.
- Pre/SOC cohort (143 pts) vs. Post/SOC+CT cohort (104 pts)
- CT protocol: Dry head CT, CTA chest, venous phase CT abd/pelvis
- In pre/SOC group, CTs ordered by treating docs in 52% (one or mix of the above CTs)
Outcomes After Protocol (Pre- vs. Post-):
- Increased identification of OHCA diagnosis (75% vs. 92%, p = 0.001)
- In SOC + CT group, diagnosis only found by CT in 13%
- In SOC group, diagnosis only found by CT in 17%
- Faster OHCA diagnosis (14.1h vs. 3.1h, p= 0.0001)
- Fewer delays in time-critical diagnoses* (62% vs. 12%, p= 0.001) *both OHCA dx and resuscitation-related injury
- No difference in ultimate diagnosis of time-critical diagnoses, rates of AKI, or survival to hospital discharge, allergic contrast reactions (0), scan complications (0), inappropriate treatments based on CT findings (0)
Bottom Line: Early pan-CT allows for earlier definitive diagnosis and stabilization without increase in adverse events. While this earlier diagnosis does not seem to yield better survival, earlier stabilization may provide some benefits in terms of resource allocation and disposition, a notable benefit during our current crisis of staffing shortages and ED boarding.
Show References
Evaluating trauma patients at Level 3 or 4 centers, rural hospitals, and non-trauma centers is difficult. Understanding the amount of work-up to perform prior to transfer is important. Summers, et al suggest less is more when it comes to imaging. The receiving facility often repeats imaging leading to time delays, additional radiation exposure, and increased costs. Chest X-ray and FAST exam may be all that is indicated in centers that do not have the resources to care for injures identified on CT imaging prior to transfer.
Show References
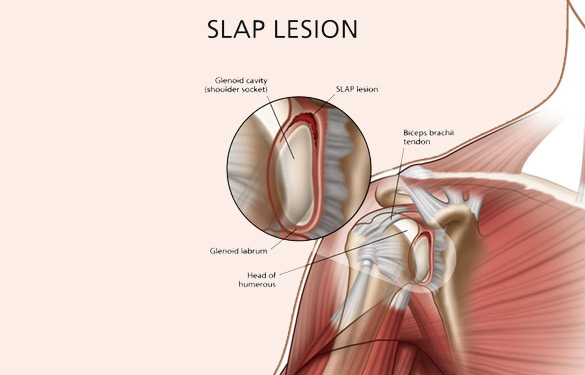
SLAP tear/lesion – Superior labral tear oriented anterior to posterior
Glenoid labrum – A rim of fibrocartilaginous tissue surrounding the glenoid rim, deepening the “socket” joint.
Integral to shoulder stability.
https://aosm.in/storage/2019/05/ch-shoulder-slap.jpg
O’Brien’s test aka active compression test for superior labral pathology.
2 parts – generally performed with the patient standing.
The patient’s shoulder is raised to 90 degrees with full elbow extension and approximately 30 degrees of adduction across the midline.
Resistance is applied, using an isometric hold.
Test in both full internal and external rotation
-This alters the position and rotation of the humerus against the glenoid
A positive test is when pain is elicited when the shoulder is in internal rotation with forearm pronation (thumb to floor) and much less or no pain when in external rotation (supination).
Note: AC joint pain may test similarly but will localize to different area of shoulder
The presence of similar, reproducible deep and diffuse glenohumeral joint pain is most indicative of a true positive test.
https://i0.wp.com/musculoskeletalkey.com/wp-content/uploads/2020/03/f50-02-9780323287845.jpg?w=960
Substance use disorder is now known to be a function of brain disease and not a moral failure. Patients with substance use disorder are highly complex and often use the ED at a higher frequency than those without the disorder. However, these patients are also frequently the target of implicit bias and stigmatizing behavior from the healthcare team that can lead to worsened outcomes. Add on top of that a racial disparity, and we can see how this group of patients can have really bad health outcomes.
This study looked at the length of time to treatment of patients with SUD, to see if there was a difference within this group based on racial or ethnic differences. It did find that black patients with SUD did wait on average 35% longer in the ED before being seen or treated. This difference was statistically significant.
While this study wasn't designed to identify the causes of such a disparity, it does raise concern for implicit bias being in effect among not only the healthcare workers, but ingrained into the healthcare systems themselves.
Patient's with SUD are a vulnerable group of patients, and black patients with SUD are experiencing a disparity in time to treatment. This should remind us all to seek out ways to remove these biases and disparities from the systems where we work.
Show References
Show References
Acetaminophen (APAP) is the leading cause of acute liver failure worldwide. Standard treatment for APAP overdose is with N-acetylcysteine (NAC), which is highly effective if given within 8 hours of ingestion. However, in delayed presenters or massive ingestions patients can still develop hepatotoxicity. Adjunctive therapies can be considered in these cases including augmented NAC dosing, renal replacement, and fomepizole.
A small amount of APAP is metabolized to N-acetyl-p-benzoquinone imine (NAPQI) by cytochrome 2E1. In therapeutic doses, the body is able to detoxify the NAPQI using glutathione. In overdose, glutathione stores get depleted and NAPQI can cause hepatotoxicity. Mitochondrial damage in APAP overdose is mediated by the c-Jun-N-terminal Kinase (JNK) pathway.
NAC works to replenish glutathione stores and detoxify NAPQI. In large overdoses, increased dosing of NAC may be necessary. Fomepizole is typically used for its alcohol dehydrogenase inhibitor property to treat methanol and ethylene glycol poisoning. Fomepizole is also a cytochrome 2E1 and JNK inhibitor and can be used in APAP overdose to block the formation of NAPQI and mitigate mitochondrial damage. Dialysis can be used to eliminate APAP from the body completely in massive overdoses or if significant acidosis or renal failure.
This study is a case series of 14 patients treated for APAP overdose between 2017 – 2021 at a tertiary hospital
- Patients treated with standard NAC therapy
- They also received IV fompeizole loading dose of 15 mg/kg followed by 10mg/kg every 12 hours at the discretion of the treating team
- Most cases received only the loading dose
- Some cases also received renal replacement therapies
- Patients had “better than expected outcomes” based on initial presentation, APAP levels, liver function tests, and expected clinical course
- No unfavorable outcomes
- No side effects
Limitations of the study:
- Patients were treated with NAC which is the standard of care
- No formal protocol for the administration or identification of patients treated with fompeizole
In summary:
- NAC is the standard of care in acetaminophen poisonings
- Consider fomepizole as an adjunctive therapy in patients that are critically ill
- Consult your poison center 1-800-222-1222 or friendly toxicologist for help in identifying these patients
Show References
Show References
Central Venous Catheter (CVC; aka central line) placement is a common procedure in both the ED and ICU, and while overall quite safe, does carry some risk. In particular, many of us regularly are confronted with the challenge of placing a line in a patient with profound thrombocytopenia, which can result in significant bleeding. In these cases, should we give platelets before we place the line?
Van Baarle et al published a randomized study in NEJM comparing an empiric 1u platelet transfusion vs no transfusion in patients with a platelet count of 10,000-50,000, prior to line placement. The study included both HD and non-HD (e.g. TLC) lines, from all three major access sites, in patients in their ICU or hematology ward. They found statistically fewer serious bleeding events in the transfusion group (4.8%) vs no transfusion group (11.9%). The study wasn't powered to look at more patient oriented outcomes like mortality, but I'm sure we can all agree less bleeding is probably a good thing. Also importantly, this study did not evaluate the risks/benefits of delaying line placement to obtain platelets when the line is urgently needed, so I would not recommend extending this to conclude platelets must be given before line placement if the line is needed for something highly time-sensitive (e.g. only available access to infuse pressors in a hypotensive patient).
Bottom Line: It is probably beneficial and appropriate to provide prophylactic platelet transfusion prior to CVC placement in patients with a platelet count less than 50,000, assuming circumstances allow.
Show References
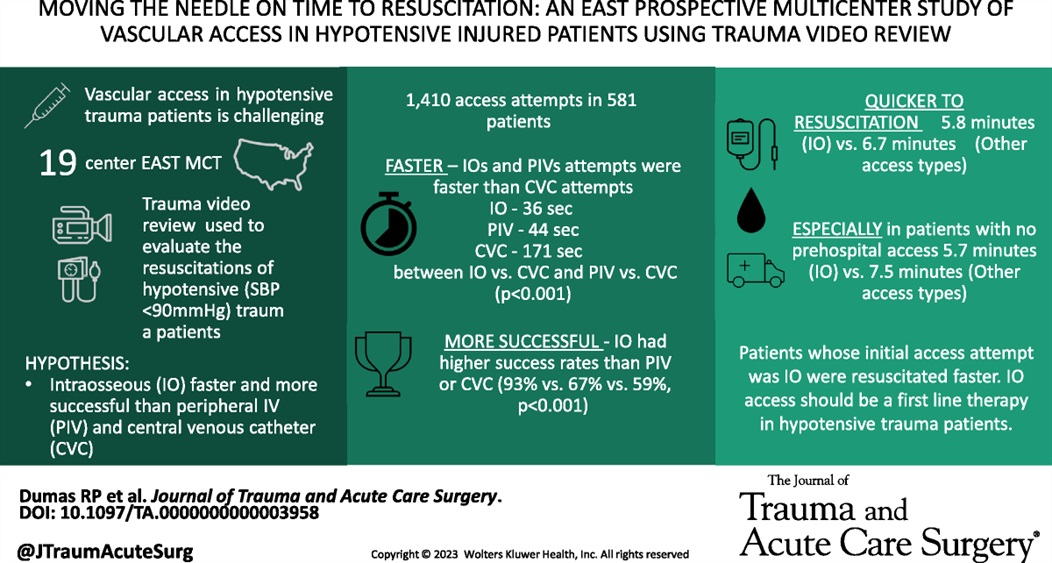
This study found that time to intraosseous was faster than time to peripheral IV. This lead to quicker resuscitation time. This was particularly true in pateints that arrived without a pre-hospital IV.
Show References
This study attempts to answer the age old question: What is the importance of fever in pediatric illnesses?
The authors' goal was to assess if response to antipyretics was associated with bacteremia. This article retrospectively reviewed 6,319 febrile children in whom blood cultures were sent and found that 3.8% had bacteremia. They then looked at the fever curve in response to antipyretics for these two groups in the emergency department over 4 hours. The study concluded that patients with bacteremia have a higher rate of persistent fever despite antipyretics. It is important to note the limitations of this study. As this was retrospective, it is unclear what clinical findings resulted in blood cultures being sent - most febrile children did not have any drawn (23,999 were excluded for this reason). They did not assess other vital signs, and did not address other bacterial infections (UTI, cellulitis, meningitis, otitis media, etc). Additionally, while patients with bacteremia did have a higher likelihood of fever, the majority of patients in both groups had fever resolution within 4 hours, and both groups had some children with persistent fevers.
Overall, this does seem to support the decision to consider obtaining further testing in those children with a persistent fever, but also emphasizes the importance of not using fever resolution alone as support for discharge to home or exclusion of bacteremia from the differential.
Show References
Citrate is an anticoagulant added to blood products to maintain stability for storage. With the administration of large volumes of blood products, citrate binds to ionized calcium, which can cause hypocalcemia. Evidence for specific calcium administration during massive transfusion protocols is limited; however, a proposed strategy has been to administer calcium gluconate 2 grams for every 2-4 units of red blood cells.
Robinson, et al. performed a retrospective analysis attempting to determine the optimal Citrate:Ca ratio (a novel ratio created for this study) to reduce 30-day mortality. They did not find any differences in mortality; however, they found a Citrate:Ca ratio of 2-3 produced a normalized ionized calcium level with 24 hours of a massive transfusion protocol.
Based on their calculations, this would equate to supplementing 1 g of calcium gluconate for every 3 units of red blood cells given.
***Reminder: Based on the amount of elemental calcium in each gram of calcium gluconate (4.7 mEq) and calcium chloride (13.6 mEq); 3 g calcium gluconate=1 g calcium chloride.***
Bottom Line: Supplementing with calcium gluconate 1 g for every 3 units of red blood cells should be sufficient to maintain normal ionized calcium levels after a massive transfusion protocol.
Show References
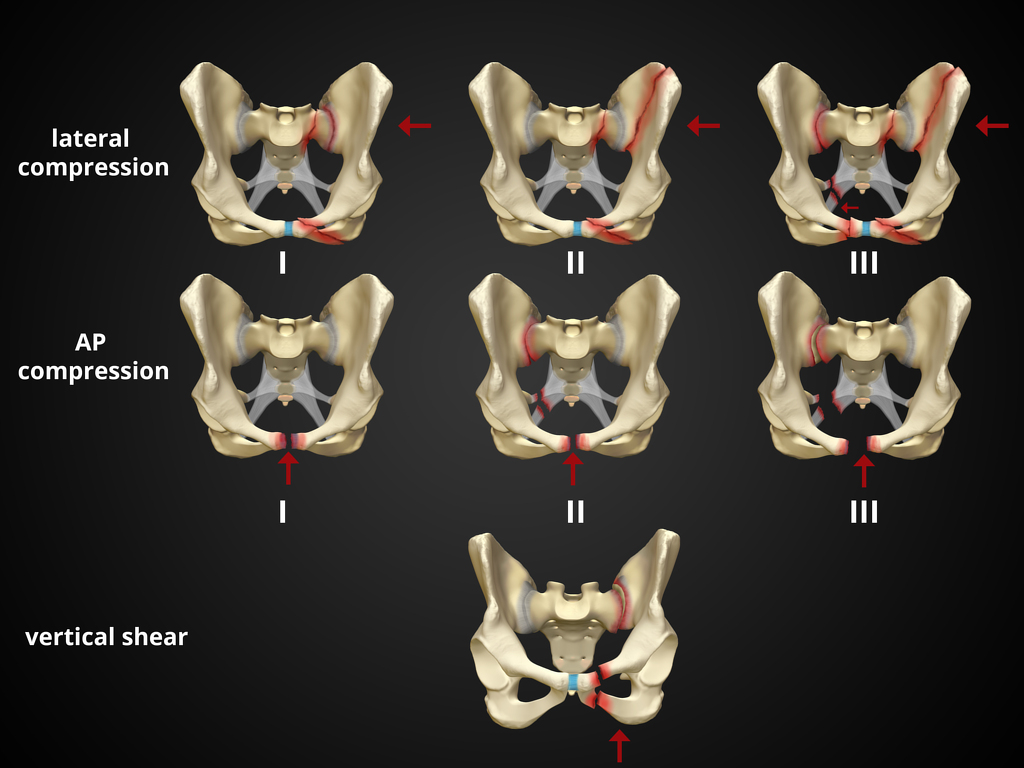
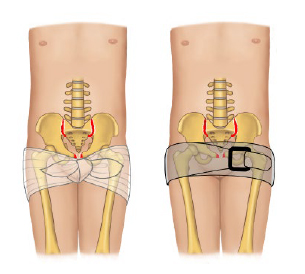
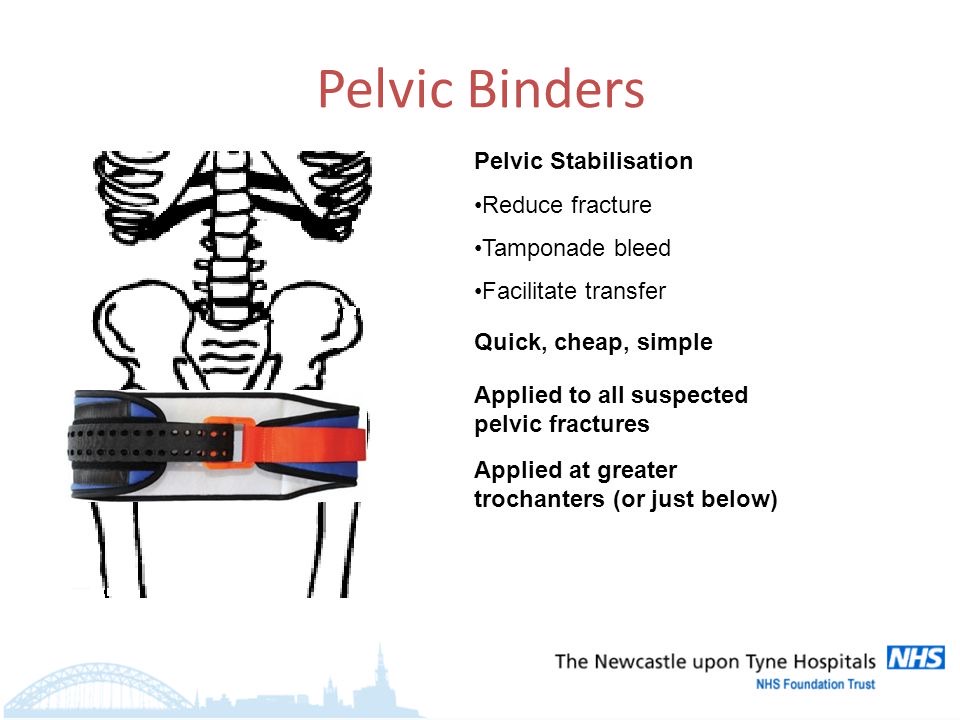
Pelvic fractures can be a major source of life threatening hemorrhage. Suspect fracture with significant force/mechanism. Signs are pelvic tenderness (no need to “rock” the pelvis), bruising at perineum, and hypotension in the setting of major trauma. Major classifications of pelvic fractures are lateral compression, anterior posterior (wide public ramus, open book), and vertical sheer (fall from height). An appropriately applied pelvic binding device can be lifesaving. The biggest mistake in applying these devices is to apply them too high. Maximum pressure is achieved with application directly across the greater trochanters.
Show References
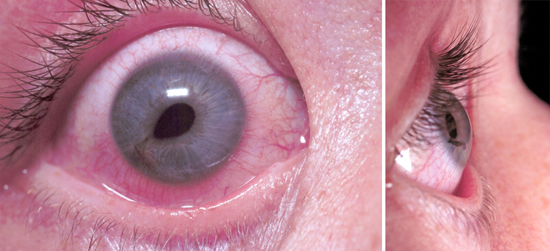
Multiple vision disorders may occur after concussion including injury to the systems that control binocular vision including: Convergence insufficiency and Accommodation insufficiency
In order to obtain a single binocular vision, simultaneous movement of both eyes in opposite directions is required.
To look at an object close by such as when reading, the eyes must rotate towards each other (convergence).
Convergence insufficiency is the reduced ability to converge enough for near vision and is a common visual dysfunction seen after concussion.
One of both eyes may also turn outward.
May lead to complaints with reading such as diplopia, blurry vision, eyestrain, and skipping words or losing one's place.
Patient or parent may also report other difficulties such as becoming more easily fatigued when reading, needing to squint and/or having disinterest in reading.
Take home: consider testing convergence in patients with some of these complaints in setting of acute or subacute head trauma.
Show References
Show References
Medical Cannabis is permitted in 39 states and Washington DC while 18 sates and Washington DC has legalized recreational cannabis use. As cannabis products become more available, pediatric exposure has also increased.
A retrospective study of National Poison Data System involving children < 6 years from 2017 and 2021 showed: Pre-COVID (2017-2019) & COVID (2020-2021)
- 7043 exposures: (increase of 1375%)
- 2017: 207
- 2021: 3054
- Residential exposure: 97% (n=6842)
Common Clinical effects
- CNS depression: 70% (n=3381)
- Pre-COVID: 61.6% --> COVID: 72.9% (p<0.05)
- Tachycardia: 11.4% (N=548)
- Pre-COVID: 10.3% -->COVID: 11.6% (p,0.05)
- Vomiting: 9.5% (n=4827)
- Pre-COVID: 7.5% -->COVID: 10.0% (p<0.05)
- Ataxia: 7.4% (n=352)
- Confusion: 6.1% (n=294)
- Mydriasis: 5.9% (n=284)
- Respiratory depression: 3.1%
Disposition
- Admission: 22.7%
- Critical care: 8.1% (n=533)
- Pre-COVID: 6.6% -->COVID: 8.6% (increase of 30%) (p<0.05)
- Non-critical care: 14.6% (n=1027)
- Pre-COVID: 9.7% -->COVID: 16.3% (increase of 68%)(p<0.05)
Conclusion
- Pediatric cannabis exposure has increased between 2017 and 2021. consequently, more pediatrics patients developing toxicity and being hospitalized.
Show References
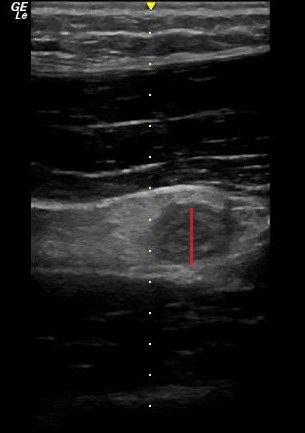
POCUS can be used to screen for appendicitis.
A recent study showed a sensitivity of 66.7% (CI 95% 47.1–82.7), and a specificity of 96.8% (CI 95% 83.3–99.9) during pregnancy, with the highest sensitivity in the first trimester.
2 methods to locate the appendix are:
1) have your patient point to the area where it hurts the most
2) perform a lawnmower technique over the right lower quadrant looking for the right psoas mucle and the iliac vessels. The appendix will usually be near these structures.
Sometimes it is easiest to use your curvilinear probe to identify an area of inflammation and then change to the linear probe for better visualization.
On ultrasound, appendicitis is defined as a non-compressible blind pouch with an outer diameter greater than 6 mm. On short axis the inflammed appendix will look like a target sign:
Show References
Shock index (heart rate/systolic blood pressure) has been used to predict trauma outcomes. This study from American Journal of Emergency Medicine looked at 89,000 pre-hospital patients who had a normal shock index on arrival at an emergency department. They then looked for those with abnormal pre-hospital shock index vs. those without an abnormal shock index and compared outcomes. Those with an abnormal pre-hospital shock index had worse outcomes than those with normal pre-hospital shock index.
Bottom line: A good handoff from pre-hospital to emergency department staff is critical because any abnormal shock index predicts a worse outcome than those with a normal shock index.
Show References
{kind=link}
{kind=link}
Author- Steve Schenkel, MD MPP Professor of Emergency Mediciner at UMEM:
A recent Annals of Emergency Medicine Publication (here https://www.annemergmed.com/article/S0196-0644(22)01276-8/fulltext) tested a predictive rule for Likelihood to Occupy an Inpatient Bed associated with a common Electronic Health Record.
At the individual patient level, the score performed ok. Depending on the chosen threshold, it traded off sensitivity and specificity and generally became more accurate the longer the patient was in the ED.
The authors and the associated editorial (here https://www.annemergmed.com/article/S0196-0644(22)01401-9/fulltext) suggest a different, potentially more beneficial use: to allow aggregate prediction of admissions across an entire department and therefore prompt earlier planning to prevent crowding on account of boarding.
The takeaway: Administrative prediction rules oriented toward individual patients may be more meaningfully used to predict resource needs, including in-patient beds, across the ED population.