Search
Myocardial Infarction in Women After Childbirth
World Health Organization reports that obesity is the 5th leading cause of global death with the highest impact on women <65 years of age
The association of obesity and cardiovascular risk in young women is currently being researched
A recent nationwide cohort looking at obesity and future cardiovascular risk looked at Danish women giving birth (2004-2009) and followed them a median time of 4.5 years
This study grouped women via pre-pregnancy body mass index (BMI)
1. Underweight (BMI <18.5)
2. Normal weight (BMI <25)
3. Overweight (BMI <30)
4. Obese (BMI >30)
Data revealed that healthy women of fertile age, pre-pregnancy obesity alone was associated with increased risk of myocardial infarction in the years after childbirth
Show References
In most situations (dependant on state laws and institutional policies), methadone-maintained patients enrolled in a drug abuse program are best managed by continuing methadone at the usual maintenance levels with once-a-day oral administration.
Pearl: In the event the methadone clinic is closed and/or the dose cannot be verified, 30-40 mg (10-20 mg IM) is generally enough to prevent withdrawal in most patients.
This is only a short-term measure and some patients may require additional methadone. Full doses of methadone should be reinstituted as soon as possible.
Show References
Case Presentation: A 63 year old woman from Texas with no recent international travel presents to the ED with persistent fatigue which onset a month ago and is associated with anorexia and occasional fevers and chills. She has been to her family doctor who tested her for a number of viral illnesses and was told she had West Nile virus.
Clinical Question:
What other febrile illness could this be?
Answer:
This patient had dengue. Dengue is now endemic in the US, and locally-acquired cases have been reported in Florida, Texas and Hawaii. The fatigue and anorexia are typical and can last for weeks after other symptoms have resolved.
West Nile virus testing may be falsely positive when another flavivirus is present such dengue, yellow fever or Japanese encephalitis.
Bottom Line:
Other possible illnesses like dengue should be considered in patients who have tested positive for West Nile virus.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
Show References
NSSTIs occur secondary to toxin-secreting bacteria; NSSTIs are surgical emergencies with a high-morbidity / mortality
Risk factors: immunocompromised host (DM, AIDS, etc.), intravenous drug use, malnourishment, peripheral vascular disease
Type I (polymicrobial; most common), Type II (monomicrobial; typically clostridia, streptococci, staph, or bacteroides), Type III (Vibrio vulnificus; seawater exposure)
Signs / Symptoms: pain out of proportion to exam (occasionally no pain at all), skin findings (blistering / bullae, gray-skin discoloration, or “Dishwater-like” discharge), or systemic toxicity (altered mental status, elevated lactate, etc.)
Diagnostic radiology
- Xray (shows gas); low sensitivity; CT scan (gas / tissue stranding); sensitivity is also low
- MRI can over-diagnose NSSTI and should not be used routinely
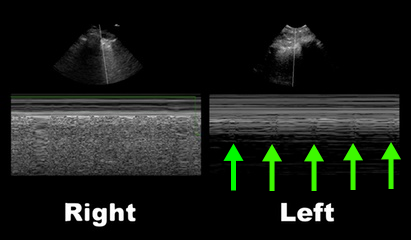
- Bedside ultrasound may demonstrate fluid or gas collections in deeper tissues (see clip below)
Treatment is emergent surgical debridement with simultaneous hemodynamic resuscitation PLUS broad-spectrum antibiotics; consider clindamycin becuase it has anti-toxin activity
Adjunctive therapies include Intravenous intraglobulin (neutralizes toxins secreted by bacteria) and hyperbaric oxygen
Show References
Question
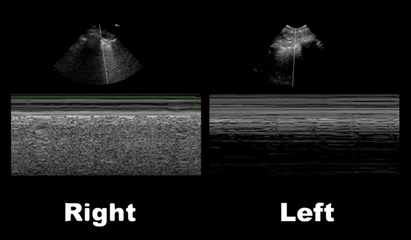
32 year-old with diabetes presents with fever, erythema, and warmth of his lower extremity; his leg is not particularly painful. He is diagnosed with cellulitis, started on antibiotics, and admitted to the hospital. While boarding in the Emergency Department he becomes rigorous and hypotensive. An ultrasound of his cellulitis is performed and is shown below. What’s the diagnosis?
Show Answer
Show References
Question
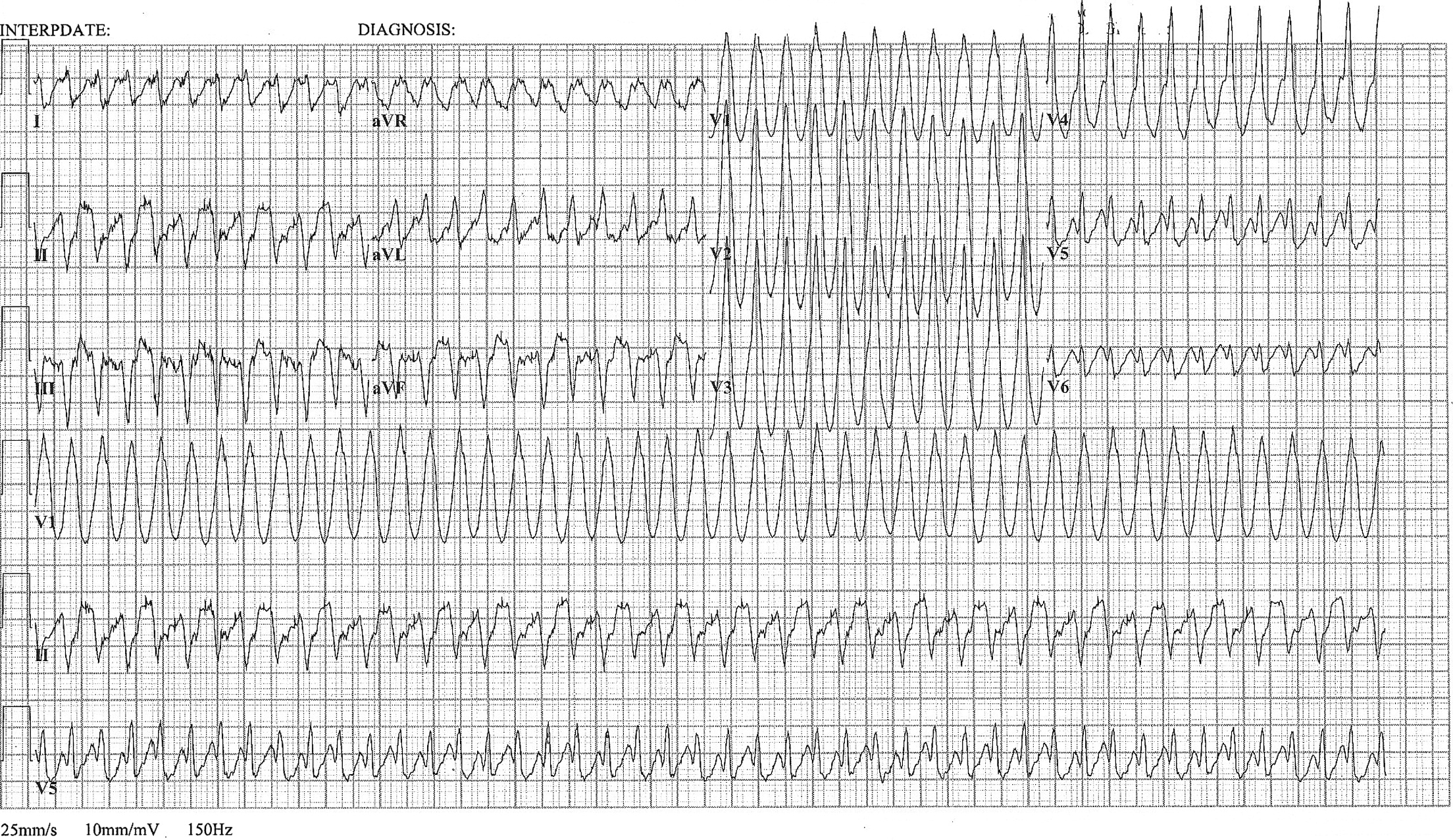
A 48 year old woman has acute chest pain and palpitations over the past several hours. She has felt similar palpitations in the past but never sought medical attention. She arrives to your ED alert and anxious. HR = 270, BP=130/100. ECG is below. What’s the diagnosis and treatment?
Show Answer
Show References
Attachments
Pelllegrini-Stieda lesion
Ossified post-traumatic lesions at the MCL adjacent to the femoral attachment site of the medial femoral condyle.
Mechanism is likely from an avulsion injury that subsequently calcifies after the initial trauma.
Often an incidental finding on plain films.
If symptomatic, refer to ortho as an outpatient
If not symptomatic, no treatment is indicated
http://images.radiopaedia.org/images/30076/b62e61e83241e30f2da693901edcdc_gallery.jpg
http://www.imageinterpretation.co.uk/images/knee/PELLEGRINI%20STIEDA2.jpg
Everyone has admitted an altered mental status, patient or bradycardic patient and all of your test results are coming back normal except for a mild increase in creatinine. Take a look at the medication list. Creatinine is a poor indicator of renal function and GFR may be severely impaired even with a mild elevation of creatinine. If you have a predominantly renally excreted drug, you can see toxic effects of a drug even if administered at therapeutic levels.
Common bradycardia inducing medication that is renally cleared: atenolol (very high renal excretion) and digoxin (70%).
Altered Mental Status and on Keppra? Keppra is 100% renally cleared!
Ask your pharmacist for help with the medication list with renal or hepatic insufficiency.
98% of venomous snake bites in the US are due to pit vipers. Occasionally a snake bite is from an exotic venomous snake being kept as a pet. In 2005, 142 exotic poisonous snakes were reported to poison control. It can be very challenging to find antivenom for these exotic animals.
Antivenom is usually specific to a family or subfamily, so the snake must be identified. Most exotic snake owners will know the common name and possibly the scientific name of the animal.
The WHO database of venomous snakes can help with identification of the species and will list antivenom available globally.
Poison centers are essential to help locate the antivenom and assist with treatment.
Relevance to the EM Physician:
When a patient presents with an exotic snake envenomation, the WHO website below can be helpful to identify the species and possible antivenom.
http://apps.who.int/bloodproducts/snakeantivenoms/database/
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg
Show References
Arterial Catheter-Related Blood Stream Infections
Whether arterial lines are a potential source of catheter-related blood stream infections (CRBSIs) is highly-debated; however, based on a recent systematic review they are an under recognized and significant source of CRBSIs.
- Incidence: In systematically cultured arterial catheters, the infection rate was 1.6 infections/1,000 catheter days which is similar to what has been reported for infections associated with short-term CVC's.
- Location: Femoral a-lines are more likely than radial a-lines to be a source of a CRBSI. Femoral a-line CRBSIs occurred in 1.5% of all catheters (95% CI, 0.8–2.2%), which is higher than radial CRBSI, with a relative risk of infection 1.94 times greater than those placed at the radial site.
- Technique: Only one study specifically evaluated the impact of full barrier precautions versus using sterile gloves only for peripheral a-lines, and it did not find any significant difference in BSI. No study has evaluated the impact of maximal barrier precautions for femoral, axillary, and brachial arterial catheters.
- Dressing: The risk of infection was significantly decreased with the use of chlorhexidine-impregnated dressings (ex: BioPatch).
Bottom Line(s)
- Arterial lines appear to be a significantly under recognized source of CRBSI's in critically-ill patients. If you are deciding to place an a-line for invasive blood pressure monitoring, strongly consider the radial site and use a chlorhexidine sponge or dressing to try and minimize the risk of future BSI.
- There is a paucity of data regarding the utility of maximal barrier techniques when inserting peripheral arterial lines. With arterial catheter infection rates approaching that of central venous catheters, we should probably be inserting a-lines with the same sterile technique.
Show References
Question
50 year-old male intubated for respiratory distress. Ultrasound is used post-intubation to confirm tube placement and the following images are obtained. What's the diagnosis?
Show Answer
Show References
Pacing Atrioventricular Block
- Atrioventricular (AV) block is classically treated with restoration of heart rate via right ventricular pacing, however high rates of right ventricular pacing is associated w/ left ventricular systolic dysfunction
- A recent multi-center randomized control trial (RCT) assessed the efficacy of right vs biventricular pacing in heart failure w/ AV block [BLOCK HF Trial]
- Primary outcomes of: morbidity, mortality, and adverse left ventricular remodeling were shown to be significantly lower in biventricular vs right ventricular pacing
- In patients with a high rate of pacing and/or an abnormally low left ventricular ejection fraction biventricular pacing may be more advantageous than conventional right ventricular pacing
Show References
Post Operative Fever is extremely common, and with the increase in same day surgery this is a common complaint presenting to the ED. The mnemonic "5Ws" are often taught to remember the causes. They are:
- Wind - Pneumonia, aspiration, pulmonary embolism, and atelectasis
- Water - urinary tract infection
- Walking - Deep Venous Thrombosis or pulmonary embolism
- Wound - surgical wound infection
- Wonder drugs - Drug fever, or infection due to indwelling lines, or a reaction to blood products
Though many surgical textbooks report that atelectasis is the most common cause of early post-operative fever, some even claiming that it is responsible for over 90% of febrile episodes in the first 48 hours after surgery; a recent review in CHEST (reference below) showed that there is no evidence to support this. We often see atelectasis in medical patients too, and few if any of them have fever. The CHEST review found that there was no clear evidence that atelectasis causes fever at all.
Pearl: Temperature >38.9C should raise concern for a true infection, where lower temperatures can be due to pulmonary embolism, DVT, drug fever, etc….
Show References
Show References
General Information:
The H’s and N’s refer to hemagglutinin and neuraminidase—two proteins on the surface of the Influenza A virus that help it attach. Here’s a quick breakdown of important emerging strains of influenza:
Avian flu:
- H5N1 (aka. Highly Pathogenic Avian Influenza A): Case Fatality Rate (CFR) 60%, no sustained person to person transmission, primarily in Asia and Middle East--first death in the Americas occurred in Canada last week (returned traveller from China)
- H7N9: new strain of avian influenza identified this year, 135 cases so far, CFR 33%, no sustained person to person transmission, found in China
Swine flu:
- H1N1: pandemic flu of 2009 making a comeback. causes more severe disease in young and middle-aged adults, predominant this season in the US (of subtyped virus tests ~98% were H1N1)
Relevance to the EM Physician:
As the frontline against the flu virus, we should know what to expect. H1N1 has predominated this flu season—so far 60% of hospitalizations occurred in patients aged 18-64, which is unusual. H7N9 is new on the scene but might be imported, and H5N1 has arrived.
Bottom Line:
Expect to see more severe illness in the 18-64 y/o age group due to H1N1. Watch for more deadly flu imports--obtain a travel history and notify the CDC of severe influenza-like illness in returned travellers.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Show References
Determination of Brain Death
- With the recent media spotlight on brain death (irreversible end of brain activity) due to a few recent cases, it would be helpful to review the definition.
- Rule out alternative causes including hypothermia, drug-induced coma, metabolic abnormalities, or severe electrolyte disturbances.
- A clear irreversible cause must be known based on history and diagnostic studies.
Clinical Examination
- Patient should be unresponsive to verbal or noxious stimulation, with the exception of spinally mediated responses.
- Absence of brainstem Reflexes
- No pupillary response
- Absent corneal reflex
- Absent gag and cough reflex
- Absent cervico-ocular reflex (Doll’s Eyes Maneuver)
- Absent vestibulo-ocular reflex (Cold Calorics)
- Apnea Testing (disconnecting the ventilator and evaluating respiratory drive)
If apnea testing cannot be performed due to instability, hypoxia, or cardiac arrhythmias, then a confirmatory test should be performed (from highest to lowest sensitivity):
- Angiography (lack of intracranial flow)
- EEG
- Transcranial Doppler
- Technetium-99 brain scan
- Somatosensory evoked potentials
There is state to state variation on who can perform the test and how many separate examinations need to be performed before brain death can be legally declared.
For a great review on some of the pitfalls in making the diagnosis and difficulties with the examination, please see the attached article.
Show References
Attachments
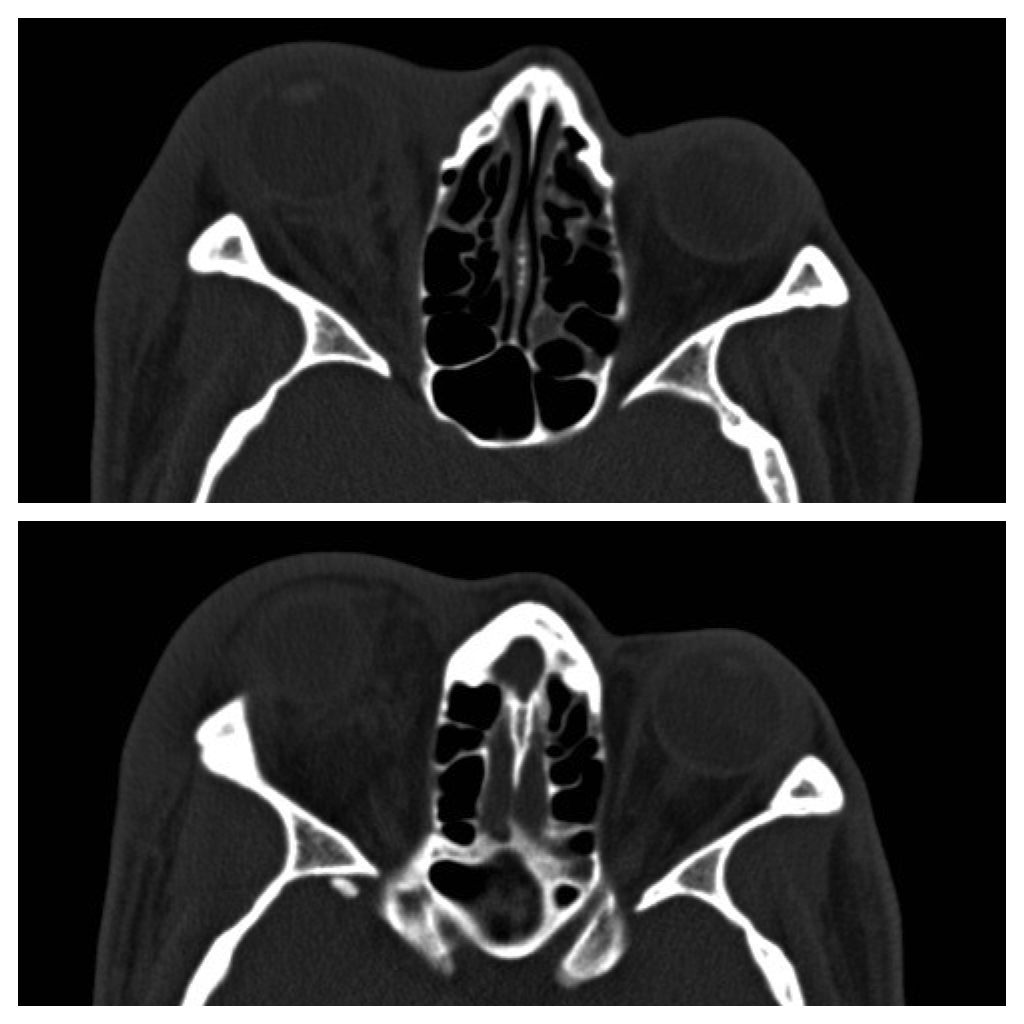
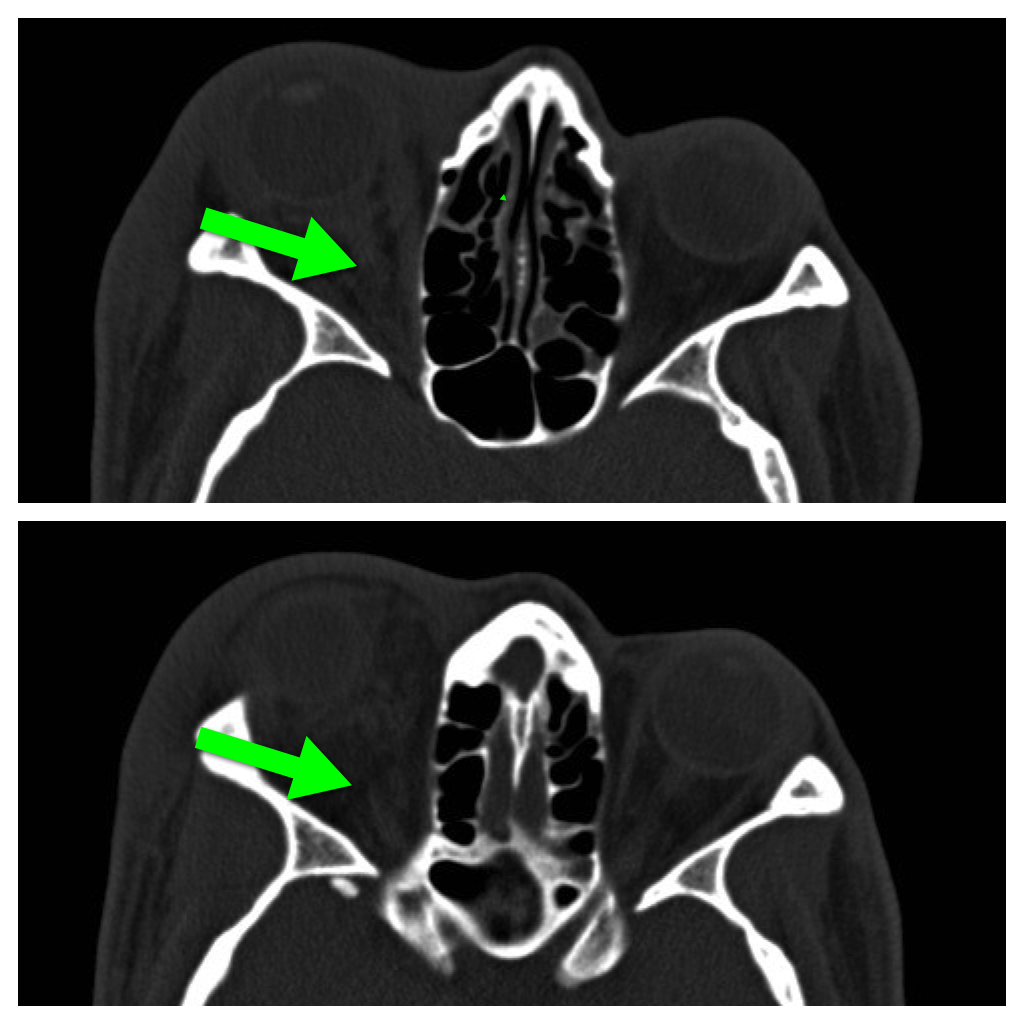
Question
42 year-old male s/p assault complains of right sided facial pain, swelling, and decreased vision. Physical exam reveals subconjunctival hemorrhage, proptosis, afferent pupillary defect, and a firm globe. What's the diagnosis and what's the emergent treatment?
Show Answer
Show References
Differentiation between right and left ventricular origin of premature beats can be useful clinically.
-
PVCs arising from the right ventricle have a left bundle branch block morphology (dominant S wave in V1)
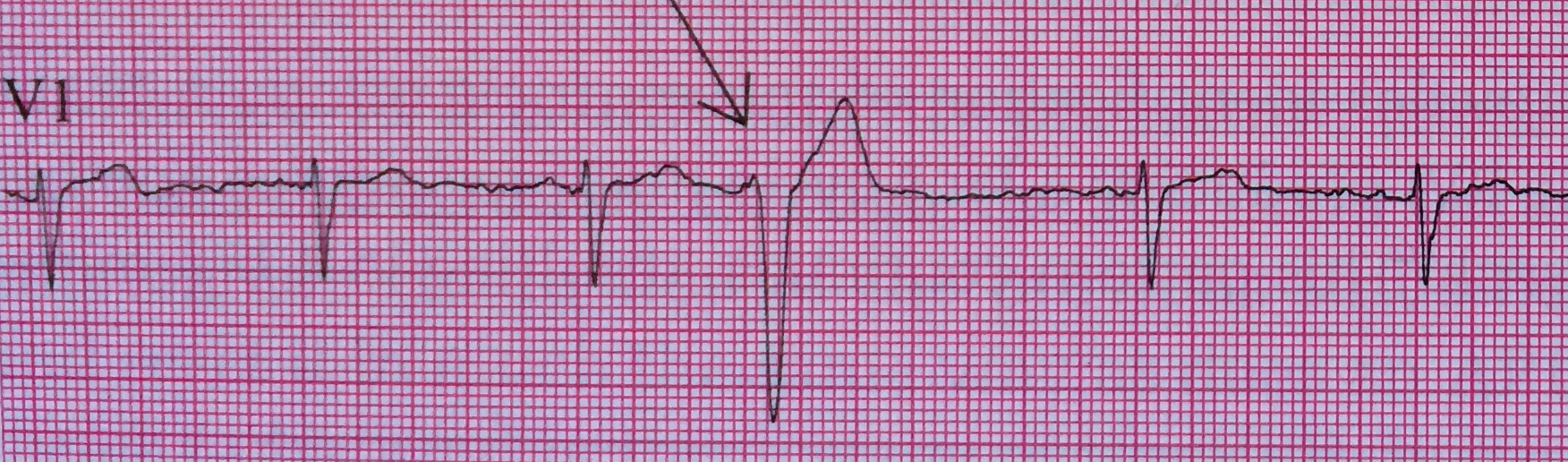
-
PVCs arising from the left ventricle have a right bundle branch block morphology (dominant R wave in V1)
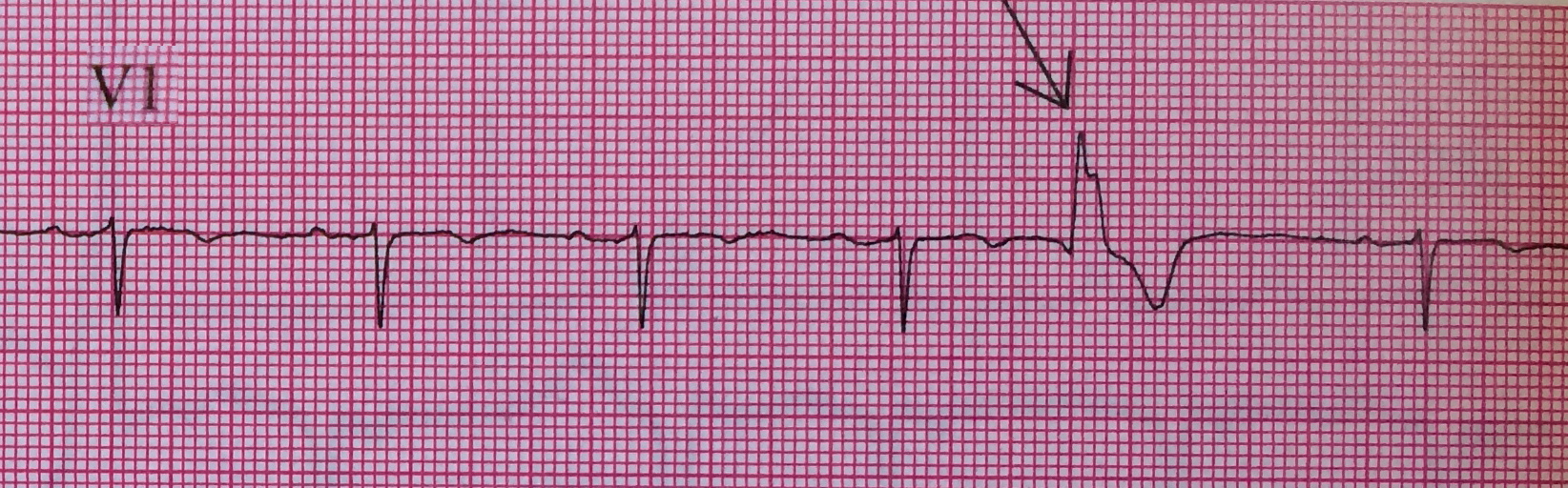
Left Ventricular premature beats are more often associated with heart disease and may precipitate ventricular fibrillation, whereas right ventricular premature beats are commonly seen in individuals with normal hearts.
Want more emergency cardiology pearls? Follow me @alifarzadmd