Search
General Information:
- 5 families of RNA viruses
- Arenaviradae – Lassa fever
- Bunyaviradae – Crimean – Congo hemorrhagic fever (CCHF)
- Hantavirus - Hemorrhagic Fever with Renal Syndrome (HFRS)
- Flaviviruses – Yellow fever, Dengue
- Filoviridae – Ebola, Marburg
- Vector transmission – humans, rodents, livestock, bush meat, mosquito, tick, contaminated feces
- Incubation of 2-14 days
Clinical Presentation:
- Mild – Mod: fever, fatigues, malaise, myalgia followed by coagulopathy (petechial rash)
- Severe: shock, coma, delirium, seizure, liver/renal failure
Diagnosis:
- Whole blood or serum can be sent to the CDC for testing (PCR, IgM/IgG, viral culture)
- Leukopenia/leukocytosis, proteinuria, thrombocytopenia, LFTs/PT/PTT, may see DIC
Treatment:
- Supportive
- Contact and airborne precautions
- Ribavirin – effective in patients with Lassa fever or HFRS (not approved by the FDA)
- Convalescent-phase plasma has been used with success in some patients with Argentine hemorrhagic fever
- FFP, high dose steroids has been reported to be successful in Crimean-Congo (CCHF)
Bottom Line:
- Immediate isolate patents with fever and signs of coagulopathy
- Supportive care primarily
University of Maryland Section of Global Emergency Health
Author: Veronica Pei
Show References
How low should you go? MAP Goals in Septic Shock
Background:
- Since Rivers’ Early-Goal Directed Therapy, a MAP of 65 mm Hg was been the standard goal for blood pressure in septic shock
- Some studies have suggested a higher target may be better for patients with hypertension
- Potentially less renal failure with a higher target
The Trial:
- 776 adult patients in France; Multi-center; randomized; non-blinded
- All patients had septic shock and on vasopressors
- MAP was maintained for 5 days or when the patient was weaned off pressors
- Primary outcome: Mortality at Day 28
- High target 65-70 mm Hg vs Low target 80-85 mm Hg
Outcome:
- No significant difference in mortality at 28 days: 36.6% (high target) vs 34% (low target) (95 %CI; 0.84 to 1.38; P=0.57)
- No significant difference at 90 days: 43.8% (high target) vs 42.3% (low target) (95% CI; 0.83 to 1.30; P=0.74)
- Incidence of newly diagnosed atrial fibrillation was higher in the high-target group
- Patients with chronic hypertension: those in the higher target group required less renal-replacement therapy
- Significant percentage of patients in the high target group did not meet goal MAP BUT the trial mirrored actual clinical practice and allowed clinicians the ability to limit blood pressure and differences in actual MAP attained in both groups was significantly different
Bottom Line:
- A MAP goal of 65 is just fine in most patients
- Patients with chronic hypertension and atherosclerosis seem to benefit (less need for renal-replacement therapies) with a higher MAP: so aim higher in these patients or monitor renal function and increase MAP goals accordingly
Show References
Question
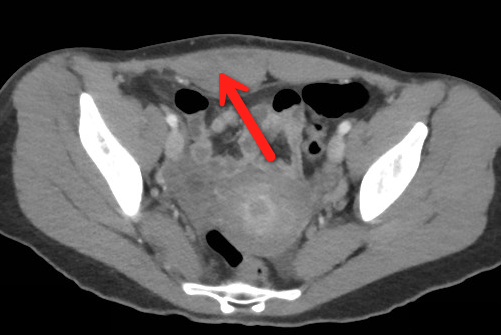
23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" pushups. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)

Show Answer
Show References
Question
23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" pushups. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)
Show Answer
Sports Hernia/Athletic pubalgia
Hx: Gradually increasing lower abdominal/proximal adductor pain. Usually activity related, resolves with rest. Frequent return despite rest when sports activity resumes.
Most common in athletes who perform cutting/maneuvers in addition to frequent acceleration/deceleration. Think ice hockey and soccer.
Bilateral symptoms not uncommon.
PE: Resisted sit up with palpation of the inferolateral edge of the distal rectus may recreate symptoms. Similarly, resisted hip adduction may elicit symptoms.
If for no other reason than to make the diagnosis harder to make, valsalva induced pain may also occur.
Fluoroscopic guided injections can be helpful to isolate the site of pain generation.
First line therapy is rest, non-narcotic analgesia and physical therapy.
With surgery, >80% return to pre injury level of play.
http://atlantasportsmedicine.com/orthopedic-surgeon/wp-content/uploads/2009/11/groin-injuries.jpg
Show References
Perinatally Infected HIV & Cardiovascular Disease
*Perinatally HIV-infected adolescents are susceptible to aggregate atherosclerotic cardiovascular disease risk, but few studies have quantified risk or developed a scoring system
*A recent study of perinatally HIV-infected adolescents calculated coronary artery and abdominal aorta PDAY (Pathobiological Determinants of Atherosclerosis in Youth) scores using modifiable risk factors: HTN, HLD, smoking, obesity and hyperglycemia
*Significant predictors of a high coronary arteries and abdominal aorta scores include: male sex, Hx AIDS-defining condition, long duration of ritonavir-boosted protease inhibitor, and no prior use of tenofovir
*PDAY scores may be useful in identifying high-risk youth who may benefit from early lifestyle or clinical interventions given their trend of increased aggregate atherosclerotic cardiovascular disease risk factor burden
Show References
A new study of almost 2 million prescriptions in VA patients compared the risk of cardiovascular death or dysrhythmia in patients receiving azithromcyin, levofloxacin, and amoxicillin.
What they found
Compared with amoxicillin, azithromycin was associated with a significant increase in mortality (HR = 1.48; 95% CI, 1.05-2.09) and dysrhythmia risk (HR = 1.77; 95% CI, 1.20-2.62) on days 1 to 5, but not 6 to 10.
Levofloxacin was associated with an increased risk throughout the 10-day period. Days 1-5 mortality (HR = 2.49, 95% CI, 1.7-3.64) and serious cardiac dysrhythmia (HR = 2.43, 95% CI, 1.56-3.79). Days 6-10 mortality (HR = 1.95, 95% CI, 1.32-2.88) and dysrhythmia (HR = 1.75; 95% CI, 1.09-2.82).
Important limitations
This study did not have a comparator group of patients getting no antibiotics. Previous data suggest patients on any antibiotic (eg, penicillin) have a higher risk of death or dysrhythmia.
The supplemental index shows that patients receiving azithromycin and levofloxacin had more serious infections (eg, PNA, COPD, etc.) which may have put them at higher risk for worse outcome irrespective of antibiotic choice.
What it means
It seems azithromycin and levofloxacin may contribute to a small increase in cardiovascular mortality and dysrhythmia during their use. A previous study found this is more likely in those with existing cardiovascular disease.
Show References
- Naloxone has technically always been able to be prescribed by physicians to individual patients.
- New laws however, make it acceptable for prescribers in many states to prescribe naloxone to “third parties,” e.g parents, friends, etc. of patients, with the assumption that the overdosed patient will not be capable of administering the antidote to themselves.
- Many states are offering short 10-20 minute training sessions on how bystanders can administer the reversal agent to the patient who has overdosed.
- If prescribed, it should be prescribed to the individual who completed the training, not the intended patient, and may be written for intranasal or intramuscular administration.
- Intranasal (IN) is “off label” and an approved intranasal preparation is not commercially available, but the intramuscular preparation can be prescribed along with an atomizer device. The usual IN dose is 1 mg per nostril which may be repeated in 3-5 minutes.
Show References
Question
You are working in a clinic in Tanzania (or Baltimore, for that matter) when a 24 year old presents with this itchy rash on his feet. What's the diagnosis and what underlying systemic condition does it indicate?

Show Answer
Show References
Attachments
Coagulopathies in Critical Illness - DIC
- Disseminated intravascular coagulation (DIC) is an acquired syndrome of intravascular coagulation and is commonly encountered in critically ill patients.
- Think about DIC in the critically ill patient with oozing at vascular sites (or wounds) and the following lab abnormalities:
- Thrombocytopenia
- Prolonged PT and aPTT
- Decreased fibrinogen
- Elevated fibrin split products and D-dimer
- Guidelines for the management of DIC are primarily based on expert opinion and include:
- Treat the underlying condition (i.e., sepsis)
- Transfuse platelets if < 50,000 per mm3
- Transfuse FFP to maintain PT and aPTT < 1.5 times normal control
- Transfuse cryoprecipitate to maintain fibrinogen levels > 1.5 g/L
- The use of heparin remains controversial and cannot be routinely recommended.
Show References
Question
25 year-old female presents with the following. It seems to have occurred spontaneously and spontaneously resolves during her ED evaluation.

Show Answer

Show References
DeQuervain and Intersection Syndromes:
- DeQuervain's Syndrome (Tenosynovitis of the Abductor Pollicus Longus and Extensor Pollicus Brevis tendons) is a common disorder that has received a lot of press lately as BlackBerry Thumb or Gamer's Thumb.
- This condition can be diagnosised by the Finklestein test [Have the patient bend their thumb into the palm of their hand, and then make a fist. They should then ulnar deviate their wrist. Pain along the tendons secures the diagnosis.]
- The pain of DeQuervain's syndrome is typically along the distal end of the radius at the base of the thumb.
- Intersection syndrome is a less common disorder though closely related to DeQuervain's Syndrome
- The pain is usually felt on the top of the forearm about three inches proximal to the wrist.
- The pain from this condition is due to tenosynovitis of the Extensor carpi radialis longus and Extensor Carpi radialis brevis muscles/tendons caused by the intersection of them with the Extensor pollicus brevis and Abductor pollicus longus tendons.
- Occurs due to excessive wrist movements.
- Intersection syndrome can be seen in weight lifters, skiers, and can be seen in homeowners in the fall and winter when they rake a lot of leaves or shovel snow.
- Treatment is the similar for both conditions and consists of:
- NSAIDS
- Cortisone injections can be effective
- Thumb and wrist immobilization with a Thumb Spica Splint or Cock Up Wrist Splint
What are characteristics that increase the chance a patient is at risk for opioid-related death? A recent JAMA article begins to tackle this very issues. Baumblatt et al. found the following:
1) Patient with 4 or more prescribers had adjusted odds ratio 6.5 for opioid-related death
2) Patient with 4 or more pharmacies where they get their prescriptions aOR - 6.0
3) Patient with more than 100 mg of morphine equivalents mean per day aOR - 11.2
With the new Maryland Prescription Drug Monitoring program (PDMP) we can start looking at a patient's prescription drug use pattern. The recent JAMA article can help you identify patients at high risk to die an opioid-related death. Use the PDMP and be wary if a patient has more than 4 prescribers or pharmacies or has >100mg of morphine equivalents per day.
Show References
Question
You are evaluating a 40 year old trauma victim and see this on pelvic xray. What are you worried about?

Show Answer
Nitric Oxide appears to have NO role in ARDS
Background: The use of inhaled nitric oxide (iNO) in acute respiratory distress syndrome (ARDS) & severe hypoxemic respiratory failure has been thought to potentially improve oxygenation and clinical outcomes. It is estimated that iNO is used in up to 14% of patients, despite a lack of evidence to show improved outcomes.
Mechanism: Inhaled NO works as a selective pulmonary vasodilator which has been found to improve PaO2/FiO2 by 5-13%, but is costly ($1,500 - $3,000 per day) and increases risk of renal failure in the critically ill.
Study: A recent systematic review analyzed 9 different RCTs (N=1142) and compared mortality between those with severe (PaO2/FiO2 < 100) and less severe (PaO2/FiO2 > 100) ARDS and found that iNO does not reduce mortality in patients with ARDS, regardless of the severity of hypoxemia.
Bottom Line: Inhaled NO is an intriguing option for the treatment of refractory hypoxemic respiratory failure, however there does not appear to be a mortality benefit to justify it's high cost and potentially negative side effects. In the ED, it is important to focus on appropriate lung protective ventilation strategies (TV: 6-8 cc/kg IBW) and maintaining plateau pressures < 30 cm H2O in the initial stages of ARDS to prevent ventilator induced lung injury while awaiting ICU admission.
Show References
The number of patients with left ventricular assist devices (LVADs) is increasing and development of optimal resuscitative strategies is becoming increasingly important. Despite a lack of evidence, many device manufacturers and hospitals have recommended against performing chest compressions because of fear of cannula dislodgment or damage to the outflow conduit.
A recent retrospective analysis of outcomes in LVAD patients who received chest compressions for cardiac arrest did not support the theory that LVADs would be harmed by conventional resuscitation algorithms.
The study was a limited case series of only 8 LVAD patients over a 4 year period. All patients received compressions and device integrity was subsequently assessed by blood flow data from the LVAD control monitor or by examination on autopsy. Although more research is necessary to determine the utility and effectiveness of compressions in this population, none of the patients in this study had cannula dislodgment and half of the patients had return of neurologic function.
Show References
Ankle Syndesmosis Injuries are also called high ankle sprains as they involve trauma to the ligaments above the ankle joint
Most ankle sprains are lateral ankle sprains. High ankle sprains are relatively uncommon.
Usual mechanism: External rotation injuries
Exam: Tenderness at the syndesmosis and compression of the tib/fib at the mid calf level causing syndesmosis pain (squeeze test)
Median recovery time is almost 4 times as long as a lateral ankle sprain 62days vs. 15days
Emergency department care is similar tto that of other ankle sprains but the added benefit of patient education and advice may improve overall care and follow-up.
Show References
Question
35yo M with history of rheumatic heart disease presents with fever. What disease process is suggested by the echo?
.JPG)
Show Answer
Show References
Attachments
In 2001, Rivers et al. published a landmark article demonstrating an early-goal directed protocol of resuscitation that reduced mortality in septic Emergency Department patients.
Many questions have arisen throughout the years with respect to that trial; critics have complained about the overwhelming change in clinical practice based on this one single-center randomized trial.
Challenging Rivers data are the ProCESS (Protocolized Care for Early Septic Shock) investigators, who released the results from a multi-center randomized control trial of 1351 septic Emergency Department patients; the primary end-point was 60-day mortality. Click here for NEJM article.
Patients in this trial were randomized to one of three groups:
-
Protocol-based EGDT
-
Protocol-based standard (did not require central lines, inotropes, or blood transfusions
-
Usual care (no specific protocol; care was left to the bedside clinicians)
Bottom-line: The investigators did not find any difference in mortality between patients in the three groups and comment that the most important aspects of managing the septic patient may be prompt recognition and early treatment with IV fluids and antibiotics.