Search
1-20 of 245 results with category "Visual Diagnosis"


Small Bowel Obstruction
- Although it takes about 11 minutes to diagnose SBO on ultrasound, newer studies have shown a decrease in sensitivity and specificity of SBO with 11 false negatives and 57 fall positives. So PLEASE BE CAREFUL when looking for SBO with ultrasound.
- Let’s give a shout out to one of our medical students, Alexa Van Besien, who recently took some great images of a patient with a known SBO.


Show References
Aortic Dissection
-
Ultrasound has a great specificity for aortic dissection. Remember to take a look at your aorta on all cardiac views.
-
Let’s give a shout out to Nikki Cali for diagnosing aortic dissection in a patient with a recent PE. Can you find the dissection flap in this image?

Show References
Peritonsillar Abscess
- Ultrasound can differentiate abscess vs cellulitis and has been shown to increase EP success of drainage as well as lower CT use. If you are concerned about complicated PTA with extension, use your clinical judgment.
- Let’s give a shout out to Kelsey Johnson and Karl Dachroeden who successfully identified and drained a PTA at bedside as well as Taylor Miller who had a difficult case of phlegmon vs early abscess.

Show References
Pulmonary Embolism
- In patients with high pretest probability and abnormal vital signs think about cardiac evaluation for pulmonary embolism. McConnell’s sign is most specific but can also be found in acute RCA infarct. TAPSE < 1.8 cm is also a good identifier of RV strain. Remember that patients with COPD or Pulm Htn may have RV dilation at baseline. You may also want to risk stratify patients with PE with labs as well as lower extremity dvt studies.
- Let’s give a shout out to Ashley Pickering who recently took some awesome echo images of a patient with a known saddle embolism.


Show References


Appendicitis
-
Ultrasound has a reported high specificity (97.9) for acute appendicitis in moderate to high pre-test probability of patients.
-
Let’s give a shout out to Reed Macy, who diagnosed appendicitis in a male with vomiting and abdominal pain!
Question
23 y/o otherwise healthy Male presents for approx. 3 month history of Right leg mass. It is painful with activity (deep and sharp) but not enlarging. Patient remembers a fall from a bicycle 6 months ago, with negative imaging for fracture.
What is the diagnosis?
https://plinthsandplatforms.files.wordpress.com/2016/06/screen-shot-2016-06-20-at-10-58-18-am.png
https://radsource.us/wp-content/uploads/2019/02/1E.jpg
Show Answer
Question
A ~55 year-old female with a history of ESRD and diabetes who presented to the ED with progressively worsening foot odor. An x-ray was performed. The picture below shows the right foot.
What is the diagnosis?

Show Answer
Show References
Question
33 y/o M with PMH of ETOH induced pancreatitis presents with epigastic/RUQ pain & N/V after drinking last night, per patient his usual “pancreas pain”. The nurse shows you his blood tubes because they look “milky”. Lipase 1200, Ca 6.8.
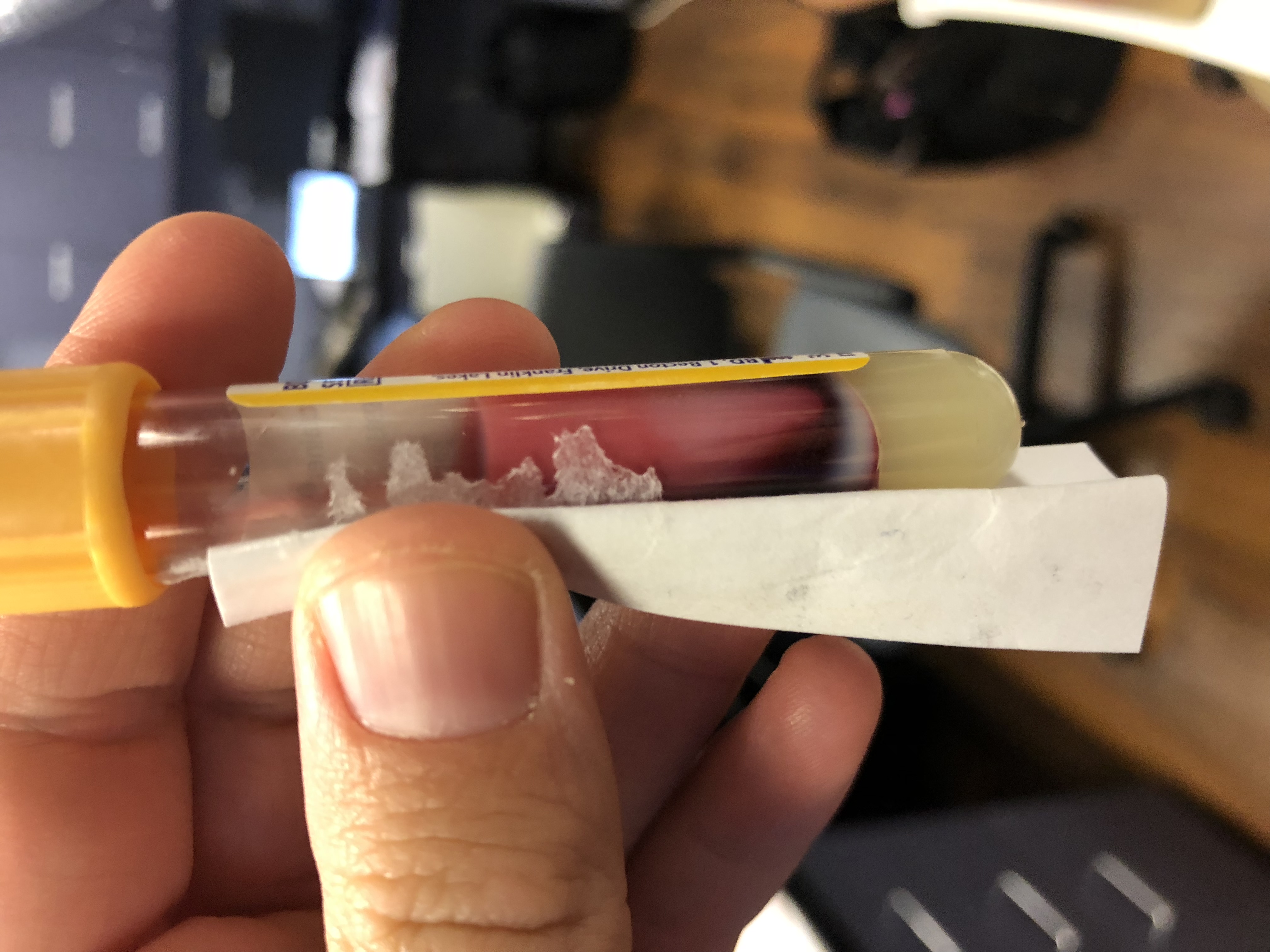
What lab test would you add?
Show Answer
Question
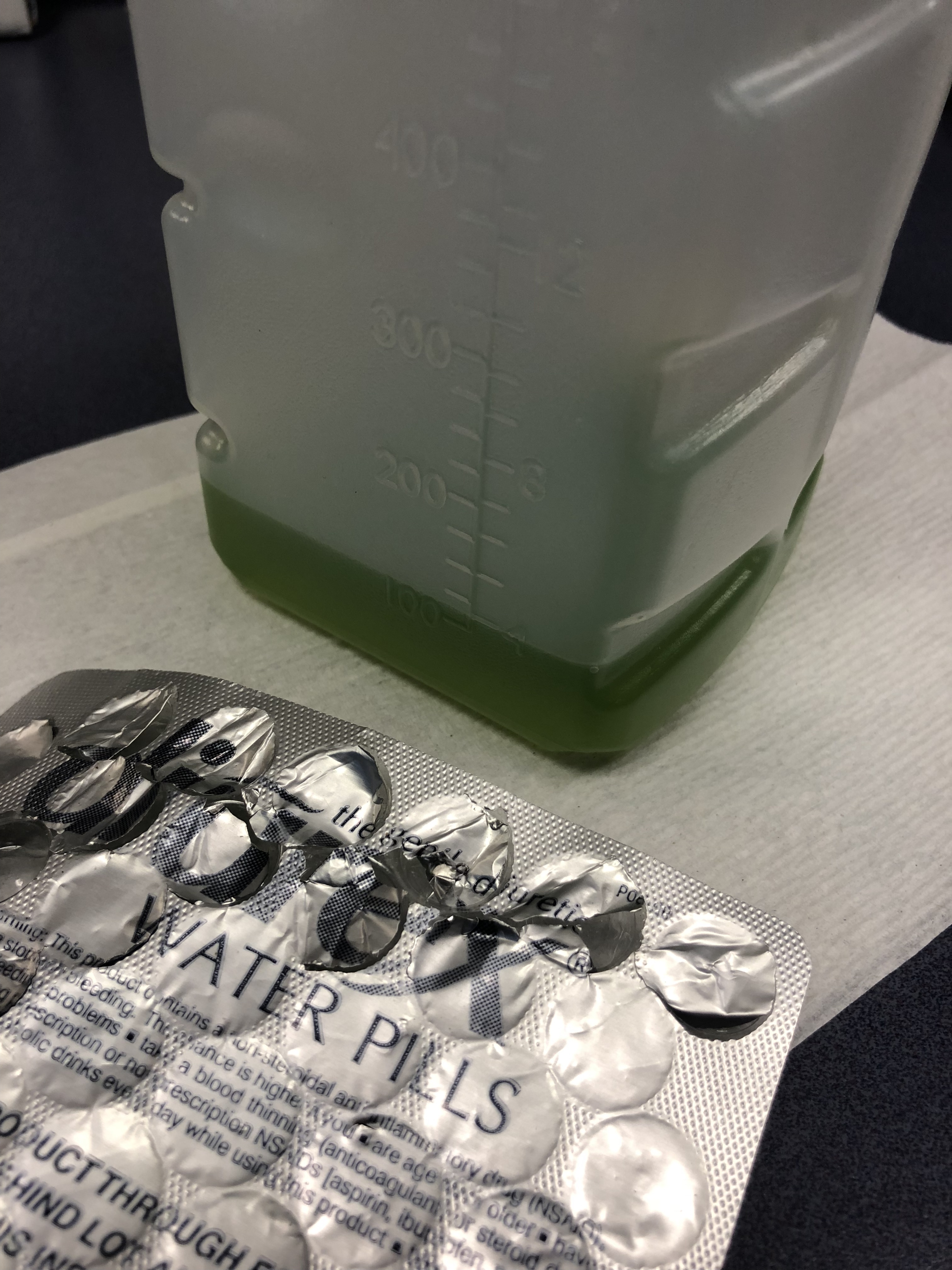
75 y/o M is brought in by EMS after he fell off the light rail and hit his head. In the ED he is A&Ox3, and is asking for a urinal. Two minutes later the tech comes running to show you the following:
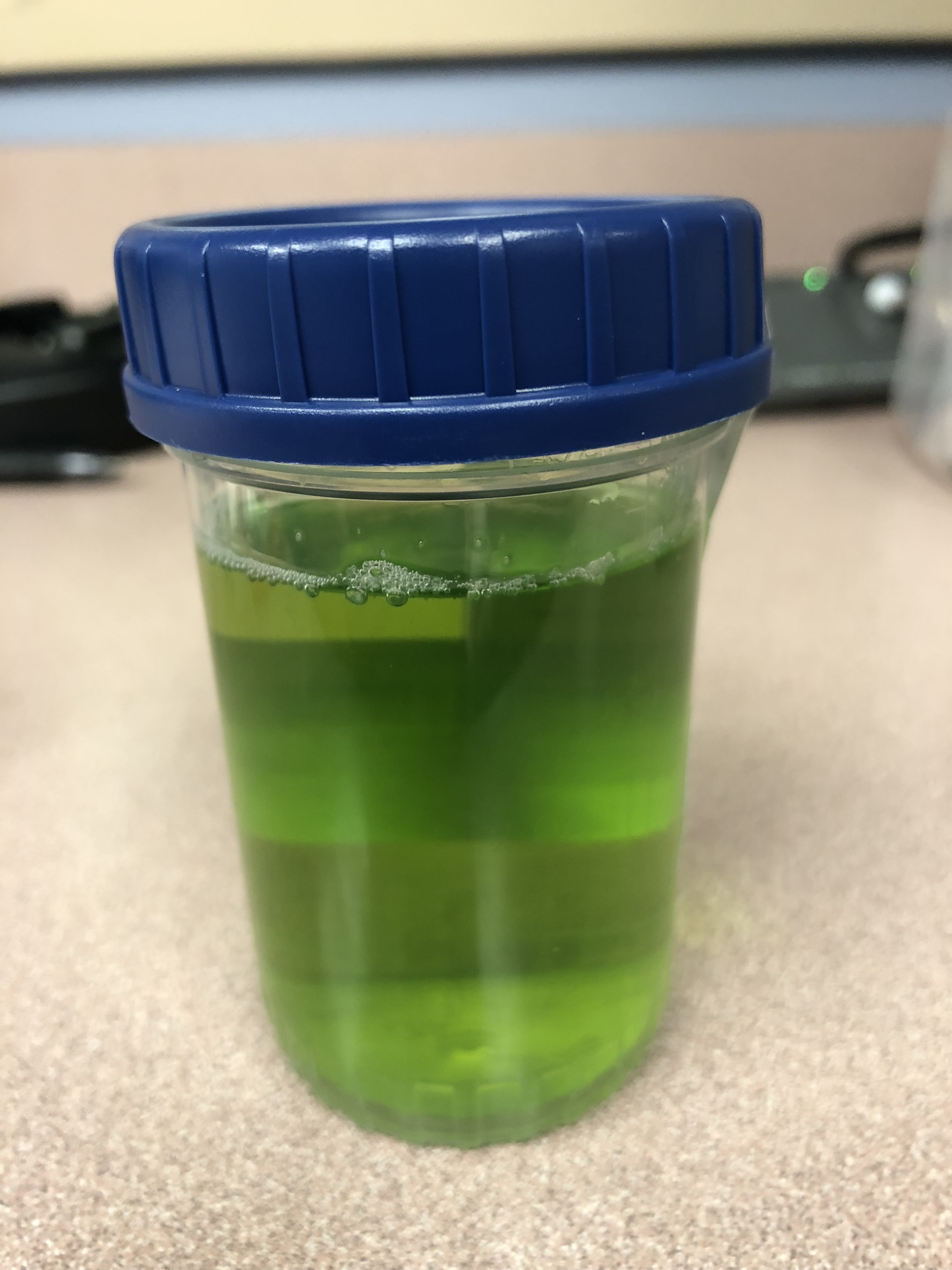
What is the cause of this patients Jolly Rancher Green Apple looking urine sample?
Show Answer
Question
A 50 years old male with a history of CHF, presenting to the ED with progressively worsening shortness of breath. POCUS was performed. The picture shows the left lower part of the chest. What is the diagnosis?

Show Answer

Show References
Question
56 year-old male with history of hypertension presents with complaints of right scrotal swelling and pain. Denies any urinary symptoms, abdominal pain, nausea/vomiting or change in bowel habits or prior episodes. Temp was 99.0.
A scrotal ultrasound was done and an image of the right testis was seen (below). What's the diagnosis?

Show Answer

Show References
Question
24-year-old male with a history of Wagner's Granulomatosis, currently on Cellcept (Mycophenolate Mofetil) and high dose prednisolone, presented with two days of sore throat, malaise and the lesions shown in the picture. What is the diagnosis?


Show Answer
Show References
Question
25 year-old female with hx of cerebral palsy with significant developmental delay, s/p G-tube who presented with acute hypoxic respiratory failure, hypotension and a distended, tense abdomen. A CT was done with the scout film below. What's the diagnosis?

Show Answer
Show References
Question
A 60 year-old man with history of atrial fibrillation, CAD presents with left lower leg/foot pain for a few days. His foot is seen below. What's the diagnosis?


Show Answer
Show References
Question
A 36-year-old male, who recently immigrated from Africa, presented to the ED with fever, rash, cough and shortness of breath. He was noted to be febrile to 39.0 C. The rash is disseminated but present mainly in his trunk as shown in the picture.

Show Answer
Show References
Question


Show Answer
Show References
Question
30 Year-old female presents to the ED for a rash. The rash started suddenly, mainly in her extremities and it is painful. The patient denied having fever or chills. Her past medical history is unremarkable. She admits to using cocaine frequently. The rash is shown in the picture.

Show Answer
Show References
Question
27 year-old G2P1 presents with 3 days of abdominal pain that is mostly suprapubic. Denies any urinary symptoms and vaginal bleeding. Physical examination reveals slight rebound in the right lower quadrant.
An ultrasound revealed the following. What's the diagnosis?

Show Answer

{kind=link}
{kind=link}
Show References
Question
A 15 months old male with no past medical history, presenting with two days of decreased oral intake and decreased urine output. The exam was notable for minimal tenderness of abdomen. During an oral fluid challenge in the ED, the patient had a single episode of bilious vomiting. The ED physician ordered an ultrasound study and the results are shown below. What is the diagnosis?
