Search
- Current ACEP guidelines recommend to consider neuroimaging after blunt head trauma in patients with coagulopathy.
- However, they do not provide guidance specific to antiplatelet vs. anticoagulant medications.
- A recent multicenter prospective observational study of 9070 patients where 14.6% were receiving antiplatelet medications or warfarin found the relative risk of significant intracranial injury was:
- 1.29 (95% CI 0.88-1.87) for aspirin alone
- 0.75 (95% CI 0.24-2.30) for clopidogrel alone
- 1.88 (95% CI 1.28-2.75) for warfarin alone
- 2.88 (95% CI 1.53-5.42) for aspirin and clopidogrel in combination
- Significant intracranial injury did not include isolated linear or basilar skull fractures or single small cerebral contusions <2 cm in diameter.
- The study only included patients who underwent neuroimaging, though the researchers also looked at 368 consecutive patients with blunt head injury who did not receive neuroimaging and did not find any missed injuries at 3-month follow-up.
Bottom Line: Patients on warfarin or a combination of aspirin and clopidogrel have increased risk of significant intracranial injury after blunt head trauma. Aspirin or clopidogrel monotherapy do not appear to be risk factors.
Show References
Cauda Equina Syndrome is a medical emergency that is considered in all patients who present to the ED with lower back pain.
Clinical presentation is variable in nature and may include some combination of lower back pain, bowel or bladder dysfunction, sexual dysfunction, saddle anesthesia with motor/sensory abnormalities.
MRI is the gold standard for diagnosis
Many of us have encountered a scenario where a patient with high clinical suspicion returns with scan negative MRI.
Studies have attempted to characterize this population.
Patients in the scan negative group had an increased prevalence of functional disorders (37% vs. 9%), functional neurologic disorders (12% vs. 0%), and psychiatric comorbidities (53% vs. 20%).
Further study is needed to characterize this association.
Hospitals may consider individualized neurologic and psychiatric referral for certain patients who are scan negative in the future.
Is scan-negative cauda equina syndrome a functional neurological disorder? A pilot study. Gibson et al., Eur J Neurol 2020, Feb 19.
Show References
Show References
With ED-boarding of critically-ill patients becoming more common, it is likely that ED physicians may find themselves caring for a patient who develops ACS – that is, abdominal compartment syndrome. While intraabdominal hypertension (IAH) is common and is defined as intraabdominal pressure > 12 mmHg, ACS is defined as a sustained intraabdominal pressure > 20mmHg with associated organ injury.
WHY you need to know it:
ACS → Increased mortality & recognition is key to appropriate management
WHO is at risk:
- Decreased abdominal wall compliance (obese, post-surgical)
- Increased intrabadominal contents (hemoperitoneum, ascites, tumor)
- Increased intraluminal contents (gastroparesis, ileus)
- Capillary leak / aggressive fluid resuscitation (sepsis, burns)
HOW it kills:
- Decreased blood flow to organs due to extraluminal pressure (mesenteric, renal, hepatic ischemia)
- Decreased diaphragmatic mobility, hypoventilation/oxygenation
- Decreased venous return, decreased cardiac output
→ Lactic acidosis, respiratory acidosis, multisystem organ failure, cardiovascular collapse & death
WHEN to consider it:
- Most patients who develop ACS are already intubated or altered – but consider in responsive patients c/o severe abdominal pain, marked distension, and SOB with tachypnea
- Intubated patients – recurrent, ongoing high pressure alarms with relatively low lung volumes, tachypnea
- Abdomen distended and minimally ballotable
- New / worsening oliguria / anuria
- Labs demonstrate increased creatinine, LFTs, lactate elevated “out of proportion” to patient presentation prior to decompensation
- Imaging may reveal underlying etiology or sequelae of ACS but cannot rule it out
WHAT to do:
- Confirm diagnosis with bladder pressure (via urinary catheter) *see cited paper for how-to in the ED*
- Emergent surgical consultation (emergent laparotomy → improved hemodynamics, organ function, & survival.
- Optimize abdominal perfusion pressure (MAP - intraabdominal pressure; recommended > 60mmHg) as much as possible:
- Adequate analgeisia and sedation, if needed, to avoid agitation
- Avoid intubation if able, to avoid the positive pressure. In intubated patients, aim for low PEEPs and plateau pressures and consider short-term paralytic
- Lower the head of bed (supine to 30mmHg) to minimize abdominal "crunch"
- Aim for intravascular euvolemia. If volume overload is a contributing factor then IVF for hypotension will worsen the ACS -- start vasopressor instaed
- Evacuate intraluminal contents if able (NGT/rectal tube for decompression, consider erythromycin/reglan, or neostigmine for colonic pseudoobstruction)
- Evacuate intraabdominal extraluminal contents if able (therapeutic paracentesis for ascites(
- Burn patients with restrictive abdominal eschar should get escharotomy
Bottom Line: Abdominal compartment syndrome is an affliction of the critically ill, is assosciated with worsened mortality, and requires aggressive measures to lower the intraabdominal pressure while obtaining emergent surgical consultation for potential emergent laparotomy.
Show References
Question
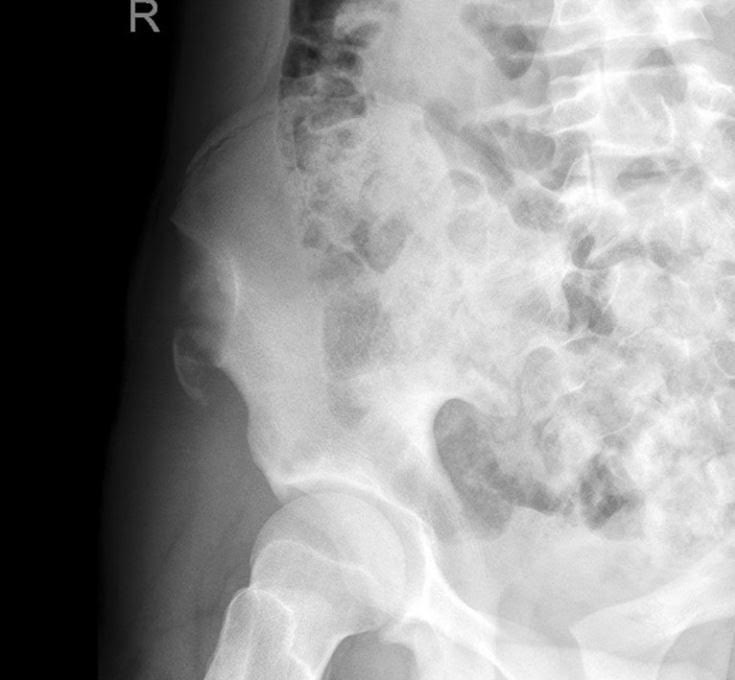
A 15 y.o. female presents to your emergency department with sudden onset hip pain after winding up to kick a soccer ball during her game today. You see a well-developed female in obvious discomfort, with tenderness to palpation over her lateral hip and pain with passive ROM at the hip. You obtain this x-ray. What is your diagnosis?
Show Answer
Show References
Metformin associated lactic acidosis (MALA) has a high rate of mortality, ranging from 25% to 50%. Lactate level and acidemia are frequently associated with poor clinical outcome in many disease/medical conditions (e.g. sepsis).
A study investigated, via meta-analysis, if lactate level and pH were predictive of mortality in MALA.
Results
44 studies were identified from PubMed, EMBASE and Web of Science.
170 cases of MALA were included
- Median age: 68.5 years
- Median pH: 7.02
- Median lactate: 14,45 mmol/L
- Overall mortality: 36.2%
pH and lactate were poor predictors of mortality based upon ROC curve
- pH: AUC of 0.430
- lactate: AUC of 0.593
Conclusion
- MALA was associated with high mortality in this meta-analysis: 36.2%
- pH and lactate were poor predictors of mortality.
- Neurogenic bladder refers to urinary tract dysfunction associated with neurological conditions.
- There are 3 patterns that can occur depending on the location of the neurological injury (see figure below):
- Suprapontine lesions (e.g. Parkinson disease) cause involuntary bladder contractions, resulting in urinary incontinence.
- Infrapontine to suprasacral lesions (e.g. cervical and thoracic spinal cord injuries) cause uncoordinated bladder and urethral sphincter contractions, resulting in incomplete emptying of the bladder and urinary retention.
- Sacral/infrasacral lesions (e.g. cauda equina syndrome) cause poor bladder contraction and/or nonrelaxing urethral sphincter, resulting in urinary retention.
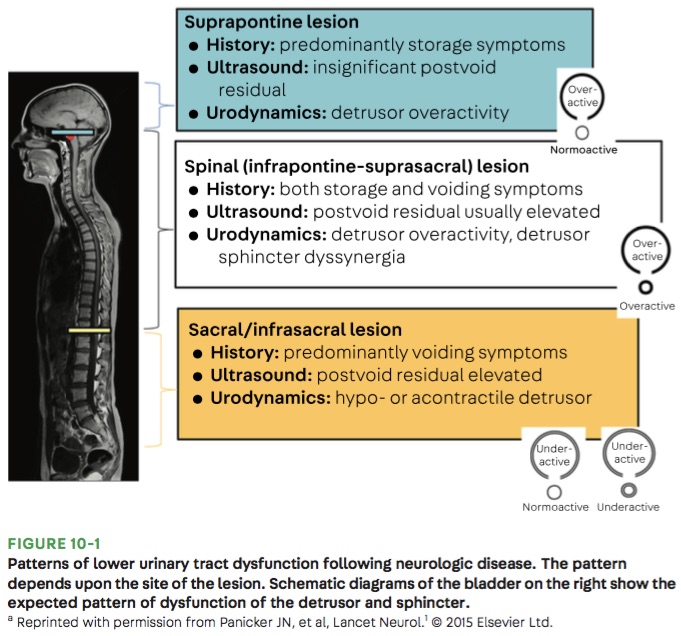
- Medications such as opiates, anticholinergics, and alpha-adrenoceptor agonists can also cause urinary retention.
Bottom Line: Urinary retention can be seen with neurological injury involving the lower brainstem, spinal cord, cauda equina, and peripheral nerves.
Show Additional Information
Show References
Don't forget cerebral fat embolism syndrome (FES) on the differential for altered trauma patients. FES is typically associated with long bone fractures, but has been reported with other fractures, orthopedic reaming (i.e. aggressive orthopedic procedures), and in rare cases even with non-fracture (soft-tissue) trauma. Typically symptoms occur between 24 and 72 hours after injury, but there have been cases both earlier and later. Diagnosis is clinical, but MRI may be helpful, and will often show multiple cerebral white matter lesions. It is debated whether FES is truly an embolic phenomena (i.e fat molecules traveling to and blocking blood supply of organs), or rather an inflammatory response to free fatty acids in the blood stream (i.e. more of a vasculitis type pathology). Management is supportive care, but give these patients time as there can be favorable outcomes, even after prolonged coma.
Show References
Taking an accurate history to diagnose Cauda Equina Syndrome (CES)
Classic teaching is to inquire specifically about bowel and bladder function, sexual dysfunction, and/or loss of sensation in the groin.
Rather than asking about urinary incontinence, clinicians should ask specifically about difficulty passing urine, new leakage and retention.
Discussing issues related to sexual dysfunction are difficult for both clinicians and patients.
Rather than asking if there are any issues with sexual function, a more direct and informative way would be to ask if the patient has a “change in ability to achieve an erection or ejaculate” or “loss of sensation in genitals during sexual intercourse.”
Saddle anesthesia has the highest predictive value in diagnosing MRI-proven CES. Loss of sensation may be incomplete and patchy. Ask about change in sensation with wiping after a bowel movement.
Show References
The new IDSA and American Thoracic Society guidelines for community acquired pneumonia were recently released. Major updates to the guidelines include but are not limited to:
1. It is not recommended to obtain sputum cultures in routine care. Consider only in patients who are intubated or empirically being treated for hospital associated pathogens such as MRSA or P. aeruginosa.
2. Blood cultures are only recommended for severe CAP managed in the hospital or those empirically being treated for MRSA or P. aeruginosa, or prior infection with those pathogens, or hospitalized and received parenteral antibiotics in the last 90 days.
3. Test for influenza during time periods when influenza is prominent (as in our current 2020 influenza outbreak).
4. Healthy patients can receive either amoxicillin 1g TID, doxycycline 100mg BID, or azithromycin 500mg followed by 250mg daily x 4 doses.
5. Patients with comorbidities such as chronic heart, lung, liver, or renal disease, diabetes, alcoholism, malignancy, or asplenia should receive combination therapy with a beta-lactam (amoxicillin/clavulanate, cefdinir, or cefpodoxime) + azithromycin or doxycycline. If allergies preclude the use of a beta-lactam, a fluoroquinolone (levofloxacin or moxifloxacin) can be used.
6. Patient admitted for non-severe CAP can receive combination beta-lactam (ampicillin/sulbactam, or ceftriaxone) and azithromycin therapy. Patients with severe beta-lactam allergies can receive either levofloxacin or moxifloxacin).
7. It is no longer recommended to add anaerobic coverage for suspected aspiration pneumonia unless the patient is suspected to have a lung abscess or empyema. It is most likely a chemical pneumonitis and should resolve within 24-48 hours with supportive therapy.
Show References
Dr. Bryan Hayes wrote a Pearl 10/4/2013 to remind us autoimmune encephalitis can present like neuroleptic malignant syndrome.
Dr. Danya Khouja wrote a Pearl 6/28/2017 to inform us autoimmune encephalitis is associated with tumors and can be investigated with serum and CSF antibody panels.
Since those publications, the number of validated autoimmune biomarkers in these panels has increased dramatically. In 2020 we now know, autoimmune encephalitis is at least as common as infectious encephalitis.
Here is how to diagnose it
1. Suspect the diagnosis in patients with subacute/rapidly progressive altered mental status, memory loss, or psychiatric symptoms. It can be mistaken for a new diagnosis of schizophrenia or bipolar disorder.
2. Look for one or more additional findings: new seizures, focal CNS findings, CSF pleocytosis, MRI findings
3. Exclude other likely etiologies (but try not to get hung up on a positive drug test, especially if drug use was not recent).
Why is this important?
Early treatment with steroids and plasmapheresis can prevent progression of disease (prevent seizures, prevent months-long hospitalizations).
Young girls are especially likely to have teratomas as a cause for the disease. Finding and resecting those tumors is life-saving.
Show Additional Information
Show References
Timeliness of Concussion Referral
Do patients with a self-limited diagnosis of “concussion” require specialty follow up?
If so, is there a benefit to earlier evaluation?
Recently published research from the University of Pittsburgh Sports Medicine Concussion Program suggests so.
Subjects: 162 concussed athletes between the ages of 12 and 22
Findings: Athletes treated in the first week after injury recovered faster than those who did not receive care until 8 to 21 days post injury.
Note: Once in care the length of time spent recovering was the same for both groups. This suggests that the amount of time prior to the initiation of care may explain the longer recovery time of the 2nd group.
Earlier recovery can help minimize effects on mood, quality of life and lost time in school/work.
Take home: Consiuder early follow up referral to a qualified provider for all concussed patients seen in the ED
Show References
Intentional drug overdose (IDO) can lead to significant morbidity and can increased patient's risk of death. A study was recently performed to identify the predictors of death in a cohort of patient who intentionally overdose on drug(s).
National Self-Harm Registry and National Drug-Related Death Index were reviewed (between January 1st, 2007 and December 31st, 2014) to identify the study cohort.
Results
|
| Non fatal IDO | Fatal IDO |
| Number of cases | 63,831 | 364 |
| Incidence | 148.8/100,000 | 1.01/100,000 |
| Male | 42.0% | 55.2% |
| Age, years (median) | 35 | 44 |
| Multiple drug ingestion | 48.5% | 78.3% |
Risk of death
- 1.7 times higher in MALE compared to female
- 5 times higher in age > 45 years vs. 15-24 years
- 3 times higher in patient who ingested 2 – 5 distinct agents, 6x higher in > 6 agent vs. single agent
- 15 times higher after TCA ingestion
- 12 times higher after opioids ingestion
- 4 times higher after antidepressants or illicit substance ingestion/exposure
Conclusion
- Older age (> 45 years), male gender and ingestion of multiple agents (>2) were associated with higher risk of death from intention drug overdose.
Show References
Mechanical Ventilation Pearls for Acute Ischemic Stroke
- Patients with an acute ischemic stroke (AIS) may require intubation for various reasons.
- Two main goals of mechanical ventilation in patients with an AIS are to maintain appropriate oxygen levels and tight control of PaCO2.
- In terms of oxygenation:
- Target normoxia
- Administer O2 if the SpO2 is < 94%
- Supplemental O2 is not recommended in non-hypoxic patients
- In terms of CO2:
- Target normocapnia
- Hypercapnia increases the risk of intracranial hypertension
- Hypocapnia can worsen cerebral perfusion
Show References
Tonsillectomy and adenoidectomy (T&A) is the second most common ambulatory surgery performed in the US. Children younger than 3 years, children with craniofacial disorders or sleep apnea are typically admitted overnight as studies have shown an increase rate of airway or respiratory complications in this population.
The most common late complications include bleeding and dehydration. Other complications include nausea, respiratory issues and pain.
Post-operatively, the overall 30-day emergency department return rate is up to 13.3%. Children ages 2 and younger were more likely to present to the ED. There is significantly higher risk of dehydration for children under 4 years. Children over the age of 6 had significantly higher bleeding risk and need for reoperation for hemorrhage control.
Show References
Many patients are treated in the emergency room for non-fatal opioid overdose. However, it is unknown what proportion of these patient population experience subsequent fatality after their ED visit.
A recent study investigated the 1-year mortality rate among Massachusetts ED patients who were treated and discharged from ED for non-fatal opioid overdose.
Results
- 11,557 patients were identified between July 1, 2011 and September 30, 2015.
- There were 635 fatalities (5.5%) within 1 year in this cohort.
- Of these, 428 (67.4%) died due to opioid overdose
Of those who died,
- 130 (20.5%) died within 1 month
- 29 (4.6%) died within 2 days.
Manner of death
- Natural causes: 121 (19.1%)
- Accidental: 460 (72.4%)
- Suicide: 13 (2.0%)
- Other/pending investigation: 41 (6.5%)
Place of death
- Hospital: 310 (48.8%)
- Residence: 146 (23.0%)
- Other/unknown/nursing home: 179 (28.2%)
Conclusion
- There is high rate of fatality within 1 month (20.5%) after non-fatal opioid overdose ED visits.
- Subsequent fatal opioid overdose was observed in 428 (67.4%) of the cohort.
Show References
Settings: multicenter, double-blind, phase 3 trial (apparently vitamin D worked in phase 2 trials).
- Patients:
- 1059 patients were enrolled within 12 hours of ICU admission. The patients had to have risk factors warranted ICU admisions (pneumonia, sepsis, mechanical ventilation, shock, pancreatitis, etc.).
- Vitamin D deficiency was defined as plasma level < 20 ng/ml
- Intervention:
- 531 patients received a single oral dose of 540,000 IU of vitamin D3 within 2 hours after randomization
- Comparison
- 528 patients received placebo
- Outcome
- 90-day all-cause mortality
Study Results:
- Total SOFA score was similar in both groups (5.6 vs. 5.4).
- On day 3, mean plasma vitamin D was higher (47 ng/ml) in treatment group vs 11 ng/ml in placebo group
- 90-day all cause mortality was similar. Treatment group was 23.5% vs. 20.6% for placebo (95% CI, −2.1 to 7.9; P = 0.26).
- Vitamin D-related adverse events were similar in both groups.
Discussion:
- This trial enrolled patients early in their critical illness compared to phase 2 trial which enrolled patients after 3 days in the ICU.
- This phase 3 trial also enrolled mostly medical-related illness, whereas 75% of patients in phase 2 had either surgical or neurology-related illnesses.
Conclusion:
Early administration of high dose vitamin D did not improve 90-day all cause mortality.
Show References
Known effects and side effects of prescribed medicines may masquerade as cauda equina syndrome (CES) .
Analgesic medicines used by patients with chronic back pain may also cloud the diagnosis of CES.
Cholinergic medications (glaucoma/myasthenia) may lead to voiding issues.
Anticholinergic medications (COPD/urinary incontinence) may lead to urinary retention.
Opioids – Constipation, reduced bladder sensation
Anticonvulsants (Gabapentin/Pregabalin)- Urinary incontinence
Antidepressants (Amitriptyline) – Urinary retention, sexual dysfunction, reduced awareness of need to pass urine
NSAIDs – Urinary retention.
- 2.3 fold greater risk versus non users. Higher in those aged 45 years or older, Highest risk (3.3 fold) was observed in patients who had recently started using NSAIDs. Dose dependent association.
Show References
Adequate treatment of adrenal crisis (AC) is often delayed, even when a h/o adrenal insufficiency is known.
- most important predictor of AC is a h/o of AC
Besides refractory hypotension, also consider in pts with:
- critically ill pts with eosinophilia (cortisol typically suppresses eosinophil counts)
- cancer patients who are on check-point inhibitor immunotherapy (they can cause severe hypophysitis or adrenalitis)
- (inhaled glucocorticoids and topical creams also cause a degree of adrenal insufficiency)
Beware of triggers:
- trauma, recent surgery, even emotional stress/exercise
- recent initiation of medications that increase hydrocortisone metabolism (avasimibe, carbamazepine, rifampicin, phenytoin, and St. John’s wort extract)
- recent withdrawal of medications that decrease hydrocortisone metabolism (voriconazole, grapefruit juice, itraconazole, ketoconazole, clarithromycin, lopinavir, nefazodone, posaconazole, ritonavir, saquinavir, telaprevir, telithromycin, and conivaptan)
Treatment:
- 100 mg IV hydrocortisone STAT as a loading dose, followed by 50 mg IV hydrocortisone q6h
- can also give 40 mg IV methylprednisolone if hydrocortisone is not immediately available
- can also give 4-6 mg IV decadron instead (will preserve integrity of ACTH stim test to diagnose adrenal insufficiency if it is performed later)
Show References
Influenza is a common cause of community-acquired pneumonia and invasive bacterial coinfection may occur. In addition, secondary bacterial pneumonia due to MRSA is becoming more prevalent. Due to the higher incidence of MRSA, it is recommended that antibiotics with activity against MRSA (vancomycin or linezolid) be included in the empiric treatment regimen, especially if the patient is critically ill.
Take Home Point: Don’t forget to add MRSA coverage to your empiric treatment regimen in those influenza patients with severe disease or secondary bacterial pneumonia.