Search
Vasopressors are used in shock-states to increase mean arterial pressure (MAP) and improve distal tissue perfusion. Additionally, some agents have effects on the heart to augment cardiac output.
Receptors that vasopressors work on include:
- Alpha-1: increase arterial tone (increases MAP) and venous tone to reduce venous pooling and augment cardiac preload
- Beta-1: increase inotropy and chronotropy on heart muscle; also increases arterial tone
- Beta-2 and Dopamine: cause vasodilation but may actually be beneficial because this increases perfusion to cardiac, renal, and GI tissues.
- V1: arterial vasoconstriction to increase MAP
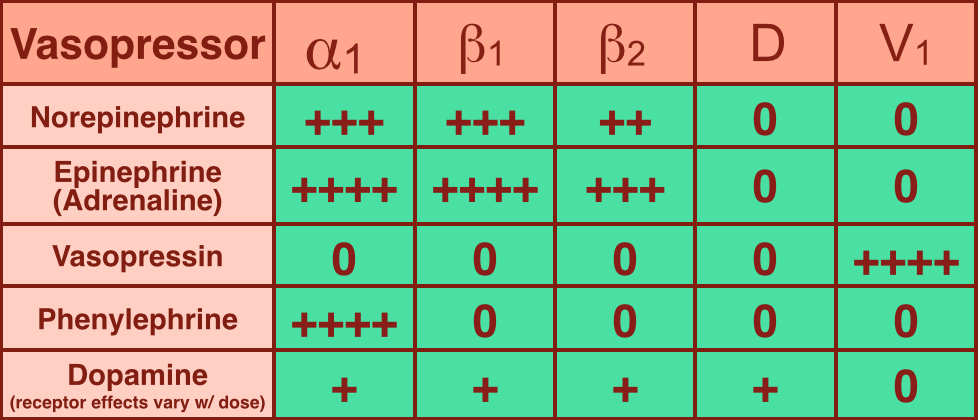
- The chart below is a summary; please note that quoted receptor effects vary depending on the source reviewed
Norepinephrine (NE): excellent vasopressor for most types of shock and recommended as a first-line agent in the Surviving Sepsis Guidelines.
- Works on alpha-1, beta-1, and beta-2 receptors.
- Initial dosing 0.05 mcg/kg/min with a maximum dose often cited as 0.5 mcg/kg/min (though there is technically no maximum dose).
Epinephrine (a.k.a. Adrenaline): in several countries the first-line agent for shock (including sepsis).
- Works similarly to NE on alpha-1, beta-1 and beta-2; it is a more potent inotrope than NE.
- One downside is the production of lactic acid, which can sometimes lead to confusion when following serial lactates during resuscitation.
References
Follow me on Twitter (@criticalcarenow) or Google+ (+criticalcarenow)