Search
There are 4 types of respiratory failure that all providers should be familiar with
Type 1: Hypoxemic, PaO2 <50; this can include shunt , V/Q mismatch, or high altitude. Pulmonary edema, ARDS, pneumonia are common causes of this type of failure.
Type 2: Hypercapnic respiratory failure; decreased RR or tidal volume. This includes neuromuscular disorders including GBS or Myasthenia Gravis, in addition to medication overdose. COPD and asthma can lead to this type of respiratory failure as well.
Type 3: Peri-operative; atelectasis; decreased FRC from being supine or obese during the operative period.
Type 4: Shock or hypoperfusion leading to increased work of breathing and respiratory failure.
The PATCH trail, recently published in the Lancet, looked at whether giving platelets to patients, that were on anti-platelet therapy (e.g.: aspirin, clopedrigrel, or dipyridamole) for at least 7 days at the time of their spontaneous intracerebral hemorrhage, improved neurologic outcomes and mortality.
This was a large (60 hospitals) multicener, open-label, masked endpoint, randomized trial that enrolled a total of 190 patients (97 platelet transfusion and 93 standard care).
The outcomes were surprising. Patient in the Platelet group had a higher rat of death or dependence at 3 months (Adjusted OR 2.05; 95% CI 1.18 3.56; p = 0.0114).
The authors concluded "Platelet transfusion seems inferior to standard care for people taking anti-platelet therapy before a spontaneous intracerebral hemorrhage"
Though this is the first study to look at this, the studies design and outcomes should really make use reconsider whether we give these patients platelets. The thought is that ICB or hemorrhagic strokes also have a component of ischemic stroke and a watershed area that's blood flow becomes compromised with the platelet transfusion.
TAKE HOME POINT: We should not routinely transfuse platelets in our patients that were on antiplatelet therapy prior to their ICB.
Show References
Show References
In consideration of the recent shootings in Orlando, Florida, how common are intentional homicides globally?
- Homicides were the 22nd leading cause of death globally in 2004
- They are projected to be the 16th leading cause by 2030
- There were an estimated 437,000 intentional homicides across the world in 2012
- This was an average global homicide rate of 6.2/100,000
- The highest regional homicide rate was in the Americas (North, Central and South) at 16.3/100,000 in 2012
- Asia had the lowest rate of 2.9/100,000
- Almost four times as many men as women die from violence each year
- However, women overwhelmingly die from intimate partner violence or from family members
Please keep the families and friends of the victims of the Orlando events, as well as the many emergency workers who helped them, in your thoughts and prayers.
Show References
Loperamide is a peripheral mu-opioid receptor agonist that is found in over the counter anti-diarrheal medication. Following the trend of opioid abuse epidemic, loperamide has been promoted on online drug-use forum as a treatment for opioid withdrawal and as a possible alternative to methadone. At the same time, recreational use of loperamide has been increasing as an opioid alternative. Unlike therapeutic use of loparamide (2 – 4 mg), loraparmide abusers take supratherapeutic doses (e.g. 50 – 100 mg) to penetrate the CNS to produce opioid effects.
In published case reports, loperamide caused cardiac Na channel blockade (similar to TCA and bupropion) and K channel blockade, resulting in EKG changes including QRS interval > 100 msec with terminal R wave in aVR and QTc prolongation, respectively. Loperamide associated death has also been reported (autopsy finding), although the exact cause of death was not determined.
It is unclear if administration of NaHCO3 can reverse the cardiac Na channel blockade as in TCA and bupropion as the clinical experiences have been limited.
Bottom line:
- Clinicians should be aware of potentially lethal cardiac toxicity of loperamide abuse (Na and K channel blockade).
Show References
Heat Stroke
- Heat stroke is critical illness defined as a core body temperature greater than or equal to 40oC and altered level of consciousness.
- Mortality from heat stroke can be as high as 30%.
- Numerous methods exist to rapidly cool patients below 39oC.
- Of these methods, ice-water immersion cools patients the fastest and is highly effective in young patients with exertional heat stroke.
- There is currently insufficient evidence to routinely recommend antipyretic agents, intravascular cooling devices, body cavity lavage, or the use of ice packs in the groin/axilla/neck. In addition, dantrolene is not recommended in the treatment of heat stroke.
Show References
Medication-overuse headache (MOH) is one of the most common chronic headache disorders
Worldwide prevalence of 1 2%
Characterized by chronic headache and overuse of different headache medications
Withdrawal of the overused medication is the treatment of choice
A 2014 study looked at adolescent patients treated in a headache clinic with chronic post traumatic headaches (concussion headaches)
77 had chronic post-traumatic headache of 3-12 months' duration
54 of 77 (70.1%) met criteria for probable medication-overuse headache.
After the OTC medicine was stopped 68.5% had resolution or improvement !!
Excessive use of analgesics postconcussion may contribute to chronic post-traumatic headaches in some adolescents.
Sometimes the advise of "just keep taking the motrin and it'll get better" isnt the answer
Show References
Ketamine is gaining traction as a prehospital option for managing severe agitation or excited delirium syndrome. Previous reports have mostly been case series, but a new prospective study adds some important information that may help delineate ketamine's role in this setting. [1] The study and an accompanying commentary are both open access. [2]
What They Did
Open-label before-and-after prospective comparison of haloperidol (10 mg IM) versus ketamine (5 mg/kg IM) for the treatment of acute undifferentiated agitation.
What They Found
- Ketamine demonstrated a statistically and clinically significant difference in median time to sedation compared to haloperidol, 5 min vs. 17 min (p < 0.0001, 95% CI: 9 15)
- Complications: ketamine, 49%; haloperidol, 5%
- Ketamine complications: hypersalivation (38%), emergence reaction (10%), vomiting (9%), and laryngospasm (5%)
- Intubation rate: ketamine, 39%; haloperidol, 4%
Appliation to Clinical Practice
- Ketamine works for prehospital agitation (and more rapidly)
- Ketamine has a higher complication and intubation rate
- Though this study did not find a dose relationship between ketamine and intubations, future studies should evaluate further and potentially use lower ketamine doses
- At our institution, we start with 2-3 mg/kg IM and repeat if necessary after 5 min. Most patients have not required a second dose and none have been intubated. This allows time to place an IV line and initiate additional treatment.
Show References
Gadolinium - To Use or Not Use?
- One advantage of MR imaging is the option between non-contrast vs. contrast-enhanced MR angiography (MRA) and venography (MRV)
- How do they work and when should you use which?
| Non-Contrast MRA/MRV | Contrast-Enhanced MRA/MRV | |
| How Does It Work? | * Time-of-flight (TOF) is a commonly used sequence * Relies on flow of blood into imaging plane * Difference between signal of blood and suppressed background tissue | * Similar to CT angiography/venography * Higher intravascular signal purely from gadolinium-based contrast, not dependent on flow
|
| Pros | * Does not require contrast
| * Generally better image quality * Shorter acquisition time |
| Cons | * Slow, turbulent, or retrograde flow may result in signal loss * Over-estimates stenosis * Longer acquisition time | * RIsks associated with contrast use * Timing of image acquisition important |
| Applications | * Patients with allergy to gadolinium, renal dysfunction, pregnancy * Evaluation of intracranial vessels and cerebral venous system | * Evaluation of stenoses and occlusions of the neck vessels and their origins at the aortic arch
|
Show References
- Current guidelines recommend IV proton pump inhibitors in setting of acute upper GI hemorrhage as a bolus + infusion (e.g. 80 mg bolus + 8mg/hr infusion).
- Recent meta-analysis comparing bolus + infusion versus intermittent bolus (most commonly 40 mg BID) demonstrated non-inferiority of intermittent bolus dosing.
- In fact, there was a trend (though not significant) to superiority of intermittent bolus dosing, with decreases in rebleeding, mortality, repeat intervention.
- From a practical standpoint, pantoprazole requires a dedicated IV line, and is not compatible with other common ICU infusions (fentanyl, propofol, norepinephrine, octreotide).
Show References
In settings where community-acquired MRSA is prevalent, which antibiotic is best for uncomplicated wound infections?
New Study
- A new multicenter, randomized, double-blind trial in 500 patients compared 7 days of clindamycin 300 mg 4 times daily to trimethoprim-sulfamethoxazole (TMP-SMX) 4 single strength tablets twice daily.
- Follow-up was performed on days 3 4 (on therapy), 8 10 (end of therapy), 14 21 (test of cure), and 49 63 (extended-follow-up).
What They Found
- Clinical cure rate was > 90% in both groups in the per-protocol population (p = 0.91), and also similar in the intention to treat populations.
- Cultured bacteria were similar between the two groups:
- MRSA ~40%
- MSSA ~25%
- Coagulase-negative staph ~15%
- Strep species ~5%
Application to Clinical Practice
- It seems like either clindamycin or TMP-SMX are appropriate antimicrobial choices in uncomplicated wound infections.
- In this study, strep species were a minor component of the total cases. TMP-SMX is generally not strong against strep species, while clindamycin has good coverage.
- Consult your local antibiogram when appropriate. At our institution, clindamycin has poor in vitro susceptibility against MRSA.
Show References
Bupropion (Wellbutrin, Zyban) is one of the most frequently prescribed antidepressants and smoking cessation agents. A lesser incidence of undesirable side effects such as weight gain and sexual dysfunction when compared to other antidepressants lends to its popularity. Bupropion's mechanism of action is only partially understood but it is known to be a norepinephine dopamine reuptake inhibitor and anticholinergic receptor blocker at certain nicotinic receptors. Bupropion has a monocyclic structure similar to amphetamines. Seizures are a major concern in overdose. When first released, Bupropion was initially withdrawn from the market due to its narrow therapeutic window with seizures occurring at doses as low as 450 mg.
- Seizures are dose dependent and all types can occur. Incidence increases dramatically with higher doses. Benzodiazepines are first-line therapy.
- Most patients experience seizure within 8 hours however, seizures can occur up to 24 hours after ingestion even without preceding symptoms.
- Longer acting forms: SR, XL, ER cause prolonged toxicity and activated charcoal should be administered in the absence of contraindications (depressed mental status, lack of airway protection, seizure).
- Myocardial sodium channel blocking properties occur and sodium bicarbonate should be administered when this occurs.
- Cardiovascular effects including tachycardia, prolonged QT interval, QRS widening, arrhythmia, and cardiovasular collapse.
- Bupropion is extremely lipid soluble and intravenous lipids should be considered in severe poisonings. Intralipid has been successfully used in several cases of Bupropion poisoning with cardiovascular instability or severe CNS symptom with good outcomes.
Show References
As we head into the summer travel season, it is important to know what potential dangers lurk out there for the unwary traveler. While injuries are usually the primary cause for death and disability for Americans abroad, what about other diseases?
The Centers for Disease Control and Prevention (CDC) has a webpage with travel health notices.
They are three types of notices:
- Warning Level 3: Avoid Nonessential Travel
- High risk to travelers
- Alert Level 2: Practice Enhanced Precautions
- Increased risk in defined settings or associated with specific risk factors; certain high-risk populations may wish to delay travel to these destinations
- Watch Level 1: Practice Usual Precautions
- Usual baseline risk or slightly above baseline risk for destination and limited impact to the traveler
Currently, there are a number of Level 1 watches and Level 2 alerts for different countries, but no Level 3 warnings. Many of the Level 2 alerts relate to Zika virus, but there are others for MERS, Yellow Fever and Polio.
To see more, go to: http://wwwnc.cdc.gov/travel/notices
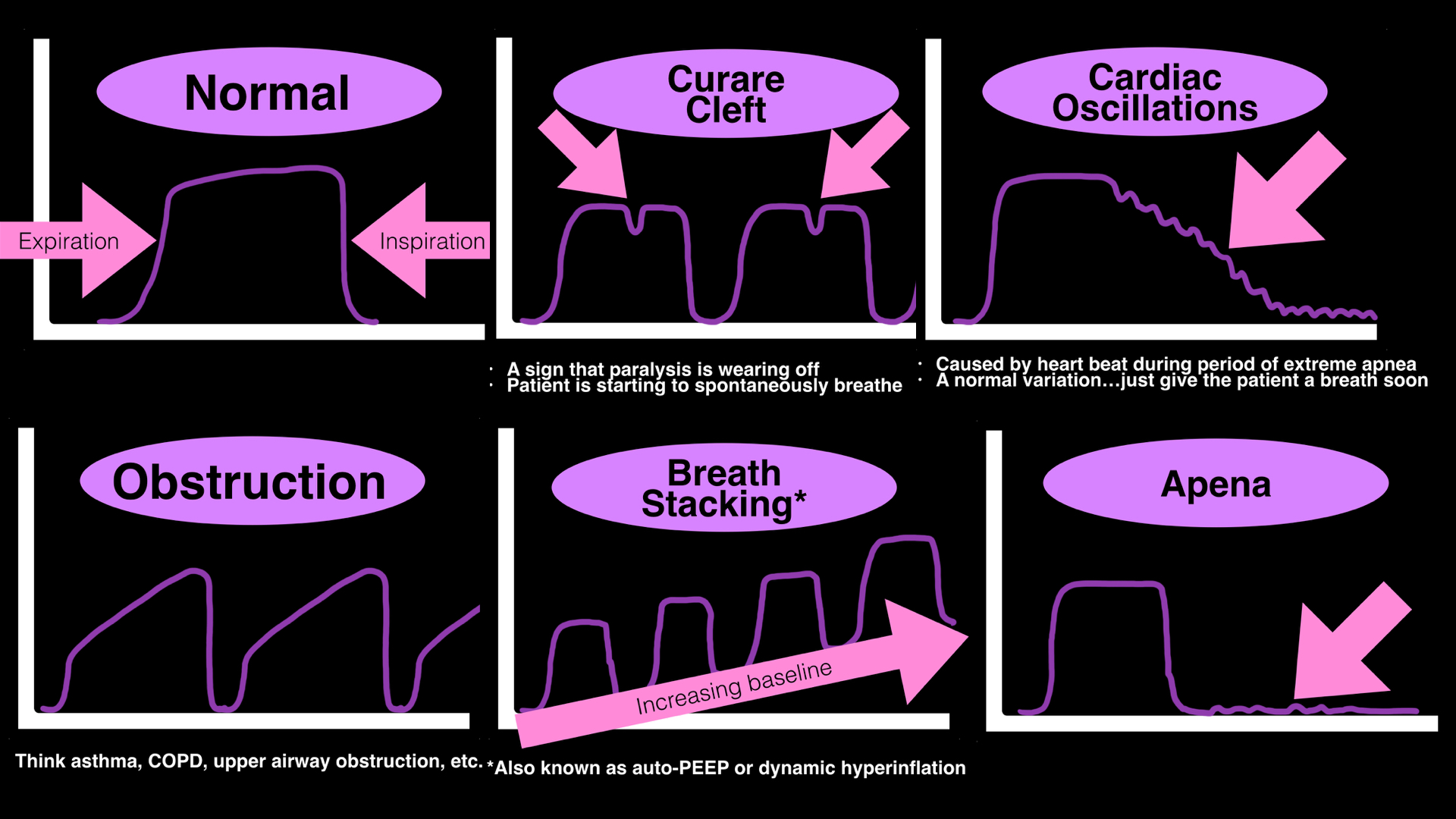
- Many clinicians use end-tidal CO2 to monitor respirations during procedural sedation or mechanical ventilation
- Typically either the presence (or absence) of a "normal" waveform or the quantitative value is used, however a lot more information can be gathered from the actual shape of the waveform; below are a few examples.
- For more examples of interpreting waveforms, click HERE.
Show References
Radiographs of the sacrum and coccyx in the emergency department (ED) have no quantifiable clinical impact, according to a study published in the American Journal of Roentgenology.
Researchers from Emory University Midtown Hospital and Morehouse School of Medicine in Atlanta, GA, sought to determine the yield and clinical impact of sacrum and coccyx radiographs performed in the ED.
Sacrum and coccyx X-rays performed on 687 consecutive patients over a six-year period in level-1 and level-2 trauma centers (4 total hospitals). The patients’ mean age was 48.1, 61.6% were women. The images were categorized as positive for acute fracture or dislocation, negative, or other.
The researchers then analyzed:
• Follow-up advanced imaging in the same ED visit
• Follow-up advanced imaging within 30 days
• New analgesic prescriptions
• Clinic follow-up
• Surgical intervention within 60 days
The researchers found positive results in 58 of the 687 patients, a positivity rate of 8.4%.
None of the 58 positive cases had surgical intervention.
There was no significant association between sacrum and coccyx radiograph positivity and analgesic prescription or clinical follow-up among the patients evaluated at the level-1 trauma centers.
However at the level-2 trauma centers, 34 (97.1%) of 35 patients with positive sacrum and coccyx radiographs received analgesic prescriptions or clinical referrals. Negative cases were at 82.9%.
Of all cases, 39 patients (5.7%) underwent advanced imaging in the same ED visit and 29 patients (4.3%) underwent imaging within 30 days.
“Sacrum and coccyx radiography results had no significant correlation with advanced imaging in the same ED visit,” the authors wrote. “There was no significant difference in 30-day advanced imaging at the level-1 trauma centers, but there was at the level-2 trauma centers.”
The researchers concluded that routine sacrum and coccyx radiography should not be part of ED practice and that patients should be treated conservatively based on clinical parameters.
Show References
Short Answer: No
Classically, some therapies for headaches are thought to be effective in only certain classifications of headaches, such as triptans in migraines, or oxygen in cluster headaches. This is not necessarily true.
Triptans have been successfully used in cluster headaches, as found in the 2013 Cochrane review.1
More recently, "high-flow" oxygen (referring to 12 L/min of oxygen, delivered through a facemask) has been studied in migraine headaches, with promising results. When compared with placebo (air), oxygen used for 15 minutes was more effective in pain relief and improving visual symptom, with no significant adverse events. 2
Show References
American Thoracic Society (ATS) Conference Highlights
The ATS conference was last week in San Francisco and a few cool articles were presented. They are briefly summarized below:
1. Using a helmet vs face mask for ARDS: Non-invasive ventilation is not ideal for ARDS for a variety of reasons. At the same time, endotracheal intubation and ventilation carries some risks as well. Could a new design of a "helmet" device make a difference? This one center study from the Univ of Chicago suggests that it would: decreased rate of intubation, increase in ventilator free days, and decrease in 90 day mortality. http://jama.jamanetwork.com/article.aspx?articleid=2522693
2. Can aspirin prevent the development of ARDS in at risk patients in the emergency department? Unfortunately, it does not appear to help. http://jama.jamanetwork.com/article.aspx?articleid=2522739
3. Should you start renal-replacement therapy (HD, CRRT etc) in critically ill patients with AKI sooner or later? Seems to have no difference and may actually lead to patients not needing any dialysis. Really a great read if you have time. http://www.nejm.org/doi/full/10.1056/NEJMoa1603017?query=OF&
4. Should I extubate at night? Lastly, probably don’t extubate at night if you can avoid it. Or just be cautious. http://www.atsjournals.org/doi/abs/10.1164/ajrccmconference.2016.193.1_MeetingAbstracts.A6150
The American Academy of Pediatrics has developed a new set of clinical practice guidelines to help better manage and think about patients who have experienced an ALTE (Apparent Life Threatening Event). The term BRUE (Brief Resolved Unexplained Event) will replace ALTE.
BRUE is defined as an event in a child younger than 1 year where the observer reports a sudden, brief and now resolved episode of one or more of: cyanosis or pallor; absent, decreased or irregular breathing, marked change in tone or altered level of responsiveness. A BRUE can be diagnosed after a history and physical exam that reveal no explanation.
BRUE can be classified as low risk or high risk. Those that can be categorized as low risk do not require the extensive inpatient evaluation that has often occurred with ALTE.
LOW risk BRUE:
Age > 60 days
Gestational age at least 32 weeks and postconceptual age of at least 45 weeks
First BRUE
Duration < 1 minute
No CPR required by a trained medical provider
No concerning historical features (outlined in the article)
No concerning physical exam findings (outlined in the article)
Recommendations for low risk BRUE:
-SHOULD: Educate, shared decision making, ensure follow up and offer resources for CPR training
-May: Obtain pertussis and 12 lead; briefly monitor patients with continuous pulse oximetry and serial observations
-SHOULD NOT: Obtain WBC, blood culture, CSF studies, BMP, ammonia, blood gas, amino acids, acylcarnitine, CXR, echocardiogram, EEG, initiate home cardiorespiratory monitoring, prescribe acid suppression or anti-epileptic drugs
-NEED NOT: obtain viral respiratory tests, urinalysis, glucose, serum bicarbonate, hemoglobin or neuroimaging, admit to the hospital solely for cardiorespiratory monitoring
*When looking at the evidence strength behind these recommendations, the only one that had a strong level was that you should not obtain WBC, blood culture or CSF
Show References
The classification of blast injuries was first described by Zuckerman in 1941 and is still widely used today. This system organizes injuries by the mechanism through which they are sustained and classifies them as primary, secondary, tertiary and quaternary. These injuries may occur in isolation or in combination with each other.
| Category | Mechanism | Typical Injuries |
| Primary | Caused by blast wave of overpressure | Tympanic membrane rupture, blast lung, intestinal hemorrhage and rupture |
| Secondary | Caused by flying debris and shrapnel | Blunt and penetrating traumatic injuries
|
| Tertiary | Due to individual being thrown by blast | Blunt and penetrating traumatic injuries
|
| Quaternary | Thermal, toxic, and asphyxiant effects | Thermal burns, chemical burns, exposure to toxins, asphyxiation
|
The term quinary blast injury has also been used to describe delayed effects of explosions, such as infections, radiation exposure, and other toxic exposures.
Author: R. Gentry Wilkerson
Show References
Situations Where ECMO Will Likely Fail
- As many EDs and ICUs begin to develop protocols for the use of ECMO, it is important to note select conditions when this therapy is unlikely to be succesful.
- Chronic respiratory or cardiac disease with no hope of recovery
- OHCA with prolonged no blood flow
- Severe aortic regurgitation
- Type A aortic dissection
- Refractoroy septic shock with preserved LV function
- Stem cell transplant patients
- Advanced age with ARDS
- Prolonged pre-ECMO mechanical ventilation (> 7 days)
- Center inexperienced with ECMO