Search
61-80 of 380 results with category "Neurology"
- CT angiography (CTA) spot sign is a strong predictor of intracerebral hemorrhage (ICH) expansion.
- However, since CTA is not part of the routine diagnostic workup of acute ICH, other predictors using noncontrast head CT have been reported in the past.
- A 5-point BAT score can be used to identify patients at high risk of hematoma expansion:
- Patients with a score ≥ 3 have a higher risk of hematoma expansion.
Show Additional Information
Show References
Patients may present atypically with ischemic strokes, reporting symptoms such as face or hemibody pain, lightheadedness, mental status change, headache and non-neurological symptoms.
Up to 25% of patients will have these symptoms.
Women are more likely than men to present with these atypical (or “nontraditional”) symptoms, especially altered mental status.
Show References
- A recent systematic review evaluated the diagnostic accuracy of 19 prehospital stroke scales.
- Arm motor strength is the most frequently evaluated item by the scales (15/19), followed by gaze (13/19) and language (13/19).
- Only 4 scales (RACE, LAMS, VAN, sNIHSS-EMS) were performed by paramedics in their original studies.
- The NIHSS, LAMS, and VAN appear to have better results in predicting large vessel occlusion.
- The presence of hemineglect, a sign of cortical involvement, improved the accuracy of the scale.
Show Additional Information
Show References
Benign headaches are common in bodybuilders. However, several less benign headaches are worth noting:
- Low cerebrospinal fluid (CSF) pressure headache: caused by a small dural tear mostly at the thoracic level. Similar to postdural headache. Treated by recumbency, and blood patches if recalcitrant.
- Subarachnoid hemorrhage (SAH)
- Spontaneous intracranial hemorrhage
- Ischemic stroke
- Dural sinus thrombosis
All except the first two are exclusively reported in patients on anabolic steroids, growth hormone, and/or “energy” supplements. Make sure to ask your patient about these risk factors.
Show References
- Greater occipital nerve (GON) block with local anesthetics is an alternate treatment option for headaches.
- Zhang et al. conducted a systematic review and meta-analysis of 7 randomized controlled trials assessing the efficacy of GON block for migraine.
- Pooled outcome suggests that GON block:
- Reduces pain intensity (mean difference -1.24 [-1.98, -0.49], p=0.001)
- Decreases analgesia medication consumption (mean difference -1.10 [-2.07, -0.14], p=0.02)
- Has no significant impact on headache duration (mean difference -6.96 [-14.09, 0.18], p=0.06)
Show References
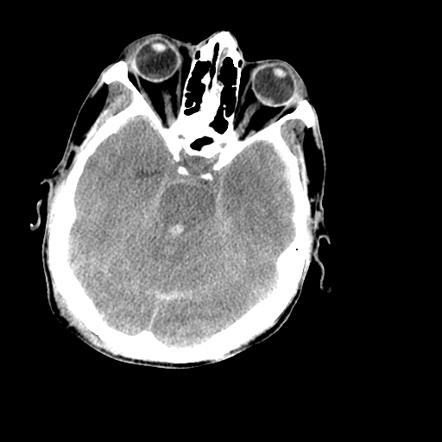
- Hyperattenuation = bright = dense (blood)
- Hypoattenuation = dark = radiolucent (fluid, air, lipid, scar)
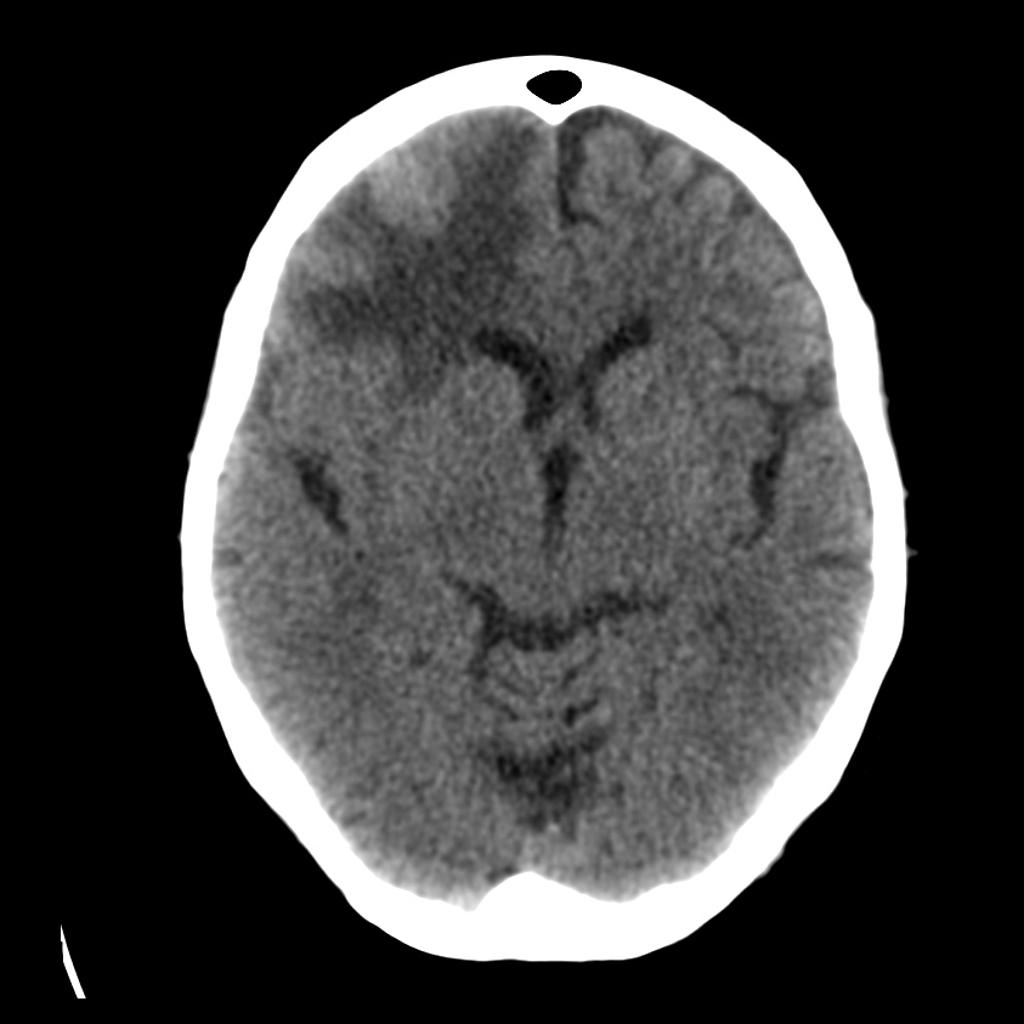
- Masses that are darker + increased volume or mass effect = edema (image 1)
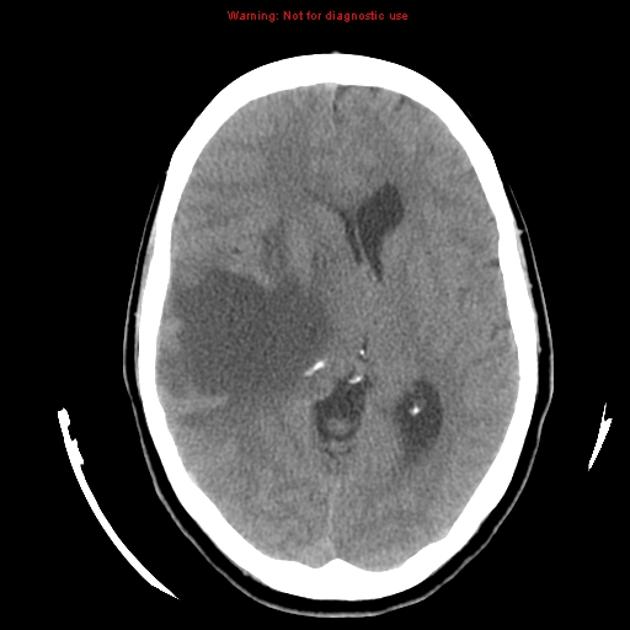
- Masses that are darker + decreased volume = scar tissue or atrophy (image 2)
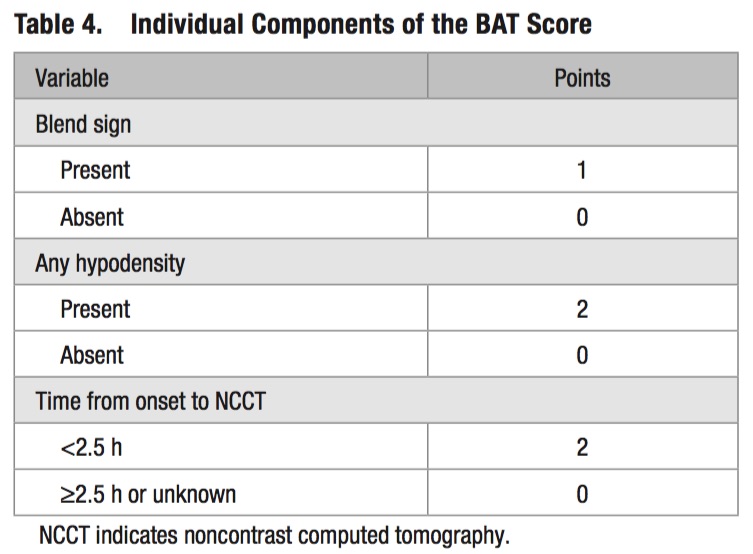
- Masses that are bright + edema = hemorrhage (image 3)
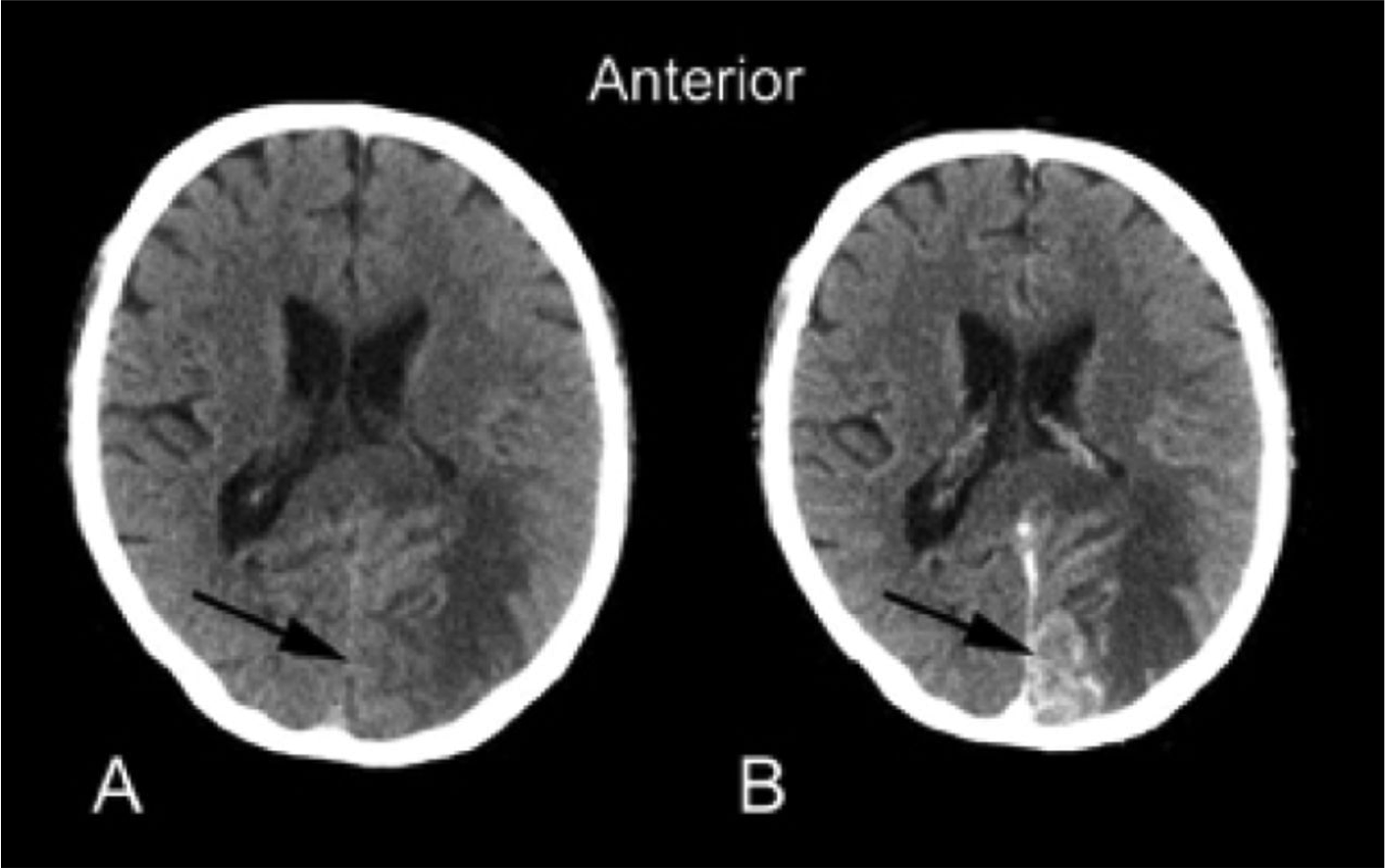
- Adding IV contrast improves detection of tumors: abnormal enhancement from disruption of blood brain barrier, necrosis or increased vascularity. (Image 4)

Show References
- Reversible cerebral vasoconstriction syndrome (RCVS) is the second most common cause of thunderclap headache after aneurysmal subarachnoid hemorrhage (SAH) and the most common cause of recurrent thunderclap headaches.
- Up to 40% of patients with RCVS have a history of migraine.
- It is associated with selective serotonin reuptake inhibitors (SSRIs), triptans, cocaine, marijuana, tacrolimus, oral contraceptives, as well as the peripartum period.
- Symptoms are often triggered by emotional stress, sexual activity, showering, straining, and physical exertion.
- Although the vasoconstriction is reversible, it can cause intracranial hemorrhage, seizures, stroke, and coma.
- Diagnosis is by history, cerebral angiography and exclusion of aneurysmal SAH.
Bottom Line: Consider RCVS in the differential of thunderclap headache and in patients who present with worse than usual migraine headache.
Show References
Show References
- The DAWN trial was a multicenter, randomized, open-label study comparing endovascular thrombectomy plus standard medical care with standard medical care alone for patients with:
- Acute stroke symptoms
- Last known well 6 to 24 hours earlier
- Evidence of intracranial ICA or proximal MCA occlusion
- Mismatch between clinical deficit and infarct volume on CTA or MRA
- The study found that patients receiving thrombectomy plus standard medical care had improved functional independence at 90 days as defined by modified Rankin Scale (mRS) of 0, 1, or 2 (49% vs 13%).
- The trial was stopped early based on prespecified interim analysis intended with the adaptive trial design.
- While the two treatment groups were similar, with median NIHSS score of 17, they had small infarct volumes and short time from symptom observation (4.8 vs 5.6 hours) compared to time of patient's last known well (12.2 vs 13.3 hours).
- 88% of the patients had unwitnessed stroke onset (including wake-up strokes), thus it is possible that these patients had actual ischemia times closer to 6 hours, thereby reproducing similar results as prior thrombectomy trials.
Bottom Line: The use of neuroimaging to identify an ischemic penumbra that may benefit from thrombectomy may be considered even for patients with time of last known well beyond 6 hours.
Show Additional Information
Show References
Show References
- A retrospective single center study reviewed 788 patients who presented to the ED with concern of stroke and found 21 (3%) patients had only aphasia symptoms by the NIHSS.
- None of these patients had evidence of infarct on neuroimaging.
- 3 of these patients were diagnosed with possible transient ischemic attack (TIA) though also had other possible diagnoses.
- Toxic/metabolic disturbances (39%), followed by seizure (11%), syncope (11%), and chronic medical problems (11%) were the most commonly diagnosed stroke mimics.
Take Home Point: This small but interesting study looked at the incidence of isolated aphasia presenting for concern of stroke. They found that none of their patients had evidence of an infarct, suggesting that strokes affecting language without motor or sensory deficits are uncommon.
Show Additional Information
Show References
It's respiratory infection and flu vaccine season! Time to brush up on Guillain-Barré Syndrome..
- It is the most common cause of acute or subacute flaccid weakness worldwide
- 70% of cases are preceded by an infection in the past 10-14 days, but most are minimized or forgotten by the patient. 40% of these infections are by Campylobacter jejuni.
- 30% develop respiratory failure requiring intubation and ventilation
- Half of the patients will develop their maximum weakness by 2 weeks, most will develop it by 4 weeks.
Show References
Traumatic brain injury (TBI) is associated with close to half of major trauma admissions in adults over age 65 in the U.K.
Falls accounted for 85% of all TBIs, while 45% of patients had subdural hematomas (SDH).
More than 3/4 of patients were treated conservatively, though outcomes were not significantly better than those who underwent neurosurgical intervention.
Higher age is associated with higher mortality and greater disability.
Bottom Line: Trauma in older adults is increasing and fall prevention is important in reducing significant injuries.
Show References
Show References
IV vs. Non-IV Benzodiazepines for Cessation of Seizures
- A meta-analysis by Alshehri et al. included 11 studies with a total of 1633 patients, comparing IV vs. non-IV benzodiazepines from any route (buccal, intranasal, intramuscular) for seizure cessation in status epilepticus.
- They found that non-IV benzodiazepine is more effective than IV benzodiazepine in patients presenting without IV access.
- The largest and highest quality study included in the meta-analysis was the RAMPART study, which was also the only study to include adults.
- When considering pediatric studies only, there is no difference between IV vs. non-IV benzodiazepine in seizure cessation for status epilepticus.
Show Additional Information
Show References
- CSF:blood glucose ratio is a useful characteristic in differentiating bacterial meningitis from viral meningitis.
- Normal CSF glucose is at least 2/3 of serum glucose level.
- In bacterial meningitis, CSF:blood glucose ratio is usually <0.4
- Rousseau et al. conducted a study comparing CSF:blood glucose ratio obtained using a bedside glucometer with the laboratory.
- They found the optimal cutoff of CSF:blood glucose ratio using a bedside glucometer is 0.46 compared to 0.44 using the laboratory.
- This proof-of-concept study suggests that a point-of-care glucometer can be used for rapid diagnosis of abnormal CSF:blood glucose ratio in the evaluation of meningitis.
Show References
- It most commonly occurs in patients with preexisting pituitary adenomas, but 3 out of 4 patients with pituitary adenomas are unaware of their diagnosis.
- Patients may acutely present with thunderclap headache, with or without visual field deficits or cranial nerve dysfunction. They may also have meningeal symptoms due to extravasation of blood into the subarachnoid space.
- Endocrine dysfunction is common but not readily diagnosed in the ED.
- Symptoms may be triggered by some hormonal treatments (e.g. GnRH agonists for prostate CA), head trauma, angiographic procedures, or anticoagulation therapy.
- CT is diagnostic in only one-third of cases, but can reveal the intrasellar mass in 80% of cases, and therefore should be the initial test. Blood may be missed in subacute cases.
- MRI is the test of choice, with a sensitivity of over 90%.
Bottomline: Keep pituitary apoplexy in your differential when considering SAH or meningitis, especially in the presence of risk factors, and have a low threshold to order an MRI.
Show References
Question
50 YOF with acute onset of worst headache of life associated with nausea and vomiting. Patient is somnolent, will rouse to noxious stimuli and complains of a headache as well as decreased vision.
Show Answer
Show References
Show References
What is the role of EEG for first-time seizures in the ED?
- Wyman and colleagues performed a prospective trial on the use of 30-minute routine electroencephalogram (EEG) in the ED after a first-time seizure or recurrent seizure without performance of a previous EEG to guide decision making in the initiation of antiepileptic medication.
- A diagnosis of epilepsy based on EEG findings was made for 21% of patients (n=15/71).
- Antiepileptic medication was initiated in 24% of patients (n=17/71), including 2 patients with abnormal but not epileptic EEG findings.
Take Home Point: A 30-minute routine EEG in the ED in adults with an uncomplicated first-time seizure revealed a substantial number of epilepsy diagnosis and can change ED management with immediate initiation of antiepileptic medication.