Search
221-240 of 380 results with category "Neurology"
- Ulnar nerve blocks are relatively easy to perform and excellent for anesthetizing the ulnar nerve distribution, particularly of the hand.
- Ulnar nerve blocks can be performed at the level of the wrist (dorsal or volar side) or at the elbow. Volar side blocks at the wrist tend to be easier to perform and associated with less risk.
- Using a 27 gauge needle, infiltrate 2 to 3 mL's of lidocaine between the flexor carpi ulnaris tendon and the distal-most aspect of the ulnar bone. The needle should be inserted 1 to 2 cm's at about a 40 degree angle, at the proximal-most wrist crease.
- Do not puncture the actual ulnar nerve or the ulnar artery. Should needle insertion cause distal hand paresthesias or blood withdrawal, do not inject and immediately remove the needle, as this suggests that the ulnar nerve or artery was struck, respectively. The objective is to allow the lidocaine to infiltrate into the nerve, not to inject it directly into the nerve.
Show References
- When examining the hand, care should be taken to thoroughly assess both the sensory and motor function on both the dorsal and palmar surfaces.
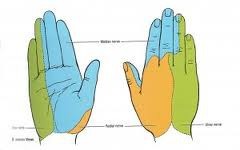
- The dermatomes of the hand provide sensation and are comprised of the ulnar, median, and radial nerves (see diagram below).
- (1) Light touch, (2) sharp touch (i.e. pinprick), (3) temperature, (4) propioception (joint position sense), (5) vibration, and (6) 2-point discrimination in the following nerve distributions should be assessed:
-- ulnar nerve >>> supplies palmar surface and dorsal tips of little finger and medial half of ring finger, including
adjacent parts of hand.
-- median nerve >>> supplies palmar and dorsal aspects of thumb, index finger, middle finger, and lateral half
of ring finger, including adjacent parts of hand.
-- radial nerve >>> supplies most of dorsal surface of hand.
- Cervicogenic headaches are a syndrome of chronic, hemicranial pain that is referred to the head from bony structures or soft tissue of the neck.
- Adequate treatment of these headaches is often difficult to achieve, particularly from the emergency department, as a multi-faceted approach including pharmacologic, physical, anesthetic nerve block, psychological and sometimes surgical therapy, is often required.
- The emergency physician may prescribe simple agents such as acetaminophen and ibuprofen, with or without muscle relaxants to treat cervicogenic headaches.
- When close follow up is ensured, low doses of tricyclic anti-depressants or anti-epileptics such as gabapentin, divalproex sodium, carbamazepine, and topiramate may be utilized; while these are not FDA approved for the treatment of cervicogenic headaches, they have been shown to be effective for some headache types and neurogenic pain syndromes.
Show References
Consider the diagnosis of a Cervicogenic Headache when the following findings are present:
A. Pain localized to the neck and occipital region, potentially with projection to forehead, orbits, temples, vertex or ears.
B. Pain is precipitated or aggravated by particular neck movements or sustained postures.
C . At least one of the following:
1. Resistance to or limitation of passive neck movements.
2. Changes in neck muscle contour, texture, tone or response to active and passive stretching and contraction.
3. Abnormal tenderness of neck muscles.
D. Radiological imaging reveals at least one of the following:
1. Movement abnormalities in flexion/extension.
2. Abnormal posture.
3. Fractures, congenital abnormalities, bone tumors, rheumatoid arthritis or other distinct pathology (not spondylosis or osteochondrosis).
Show References
Cluster headaches are defined as a group of at least five headache attacks causing unilateral orbital, supraorbital and/or temporal pain, with at least one of the following simultaneous associated findings on the affected side:
- conjunctival injection
- lacrimation
- nasal congestion
- rhinorrhea
- ptosis
- miosis
- sweating on the forehead
Cluster headaches can occur at a frequency of one every other day t eight episodes per day.
Show References
Migraine with aura (MA) diagnostic criteria
A. At least two attacks with at least 3 of the following:
1. One or more fully reversible aura symptoms (indicates focal cerebral cortical and/or brain stem functions).
2. At least 1 aura symptom develops gradually over greater than 4 minutes, or 2 or more symptoms occur in succession.
3. No aura symptom lasts greater than 60 minutes.
4. Headache follows aura with free interval of at least 60 minutes.
B. At least 1 of the following aura features establishes a diagnosis of migraine with typical aura:
1. Homonymous visual disturbance.
2. Unilateral paresthesias and/or numbness.
3. Unilateral weakness.
4. Aphasia or speech difficulty.
Show References
- Several medications such as dopamine-blocking anti-emetics, triptans, and ergotamine derivatives have been shown to more effectively treat migraine headaches over other types of headaches, making the ability to accurately recognize this common (2.2% of all ED visits) condition essential.
- According to the International Headache Society, one meets diagnostic criteria for migraine headache without aura when they have experienced at least 5 attacks, each lasting 4 to 72 hours (untreated or unsuccessfully treated) and accompanied by at least 2 of the 4 following characteristics ("PUMA"):
A.
1. Pulsatile or throbbing in quality
2. Unilateral in location
3. Moderate to severe in intensity
4. Aggravated by activity (i.e.climbing stairs, exertion), plus
B. at least 1 of the following 2 during the headache ("VP"):
1. Vomiting and/or nausea
2. Photophobia and/or phonophobia
Show References
- Lacunar infarcts affect the deep penetrating vessels of the middle cerebral artery and carry the best prognosis of all strokes.
- There are 4 classic syndromes characteristically caused by lacunar infarcts, with which the emergency physician should be familiar and able to recognize. They are:
- Pure motor hemiparesis.
- Pure sensory syndrome.
- Ataxic hemiparesis (ipsilateral cerebellar and motor symptoms).
- Clumsy hand dysarthria syndrome (ipsilateral hand weakness, patient may say their hand "feels awkward," dysarthria more pronounced than the weakness).
- The ability to detect brain CT abnormalities suggestive of ischemic stroke largely depends upon the time between the onset of symptoms and the CT examination.
- Large, cortical strokes are typically not detected on CT for at least 3 hours; Nearly 60% of strokes, however, are detectable on CT within 24 hours from time of infarct, and essentially 100% within 7 days.
- Clinical correlation: Be sure that the reported time of symptom onset properly correlates with brain CT findings, as this could affect the decision to treat with tPA in accordance with appropriate time windows. If a patient reports 1 hour of stroke symptoms, for example, and the brain CT shows significant edema and loss of gray/white matter differentiation suggesting infarct, be wary of a time discrepancy.
Show References
- Multiple Sclerosis (MS) is a relapsing condition caused by the destruction of myelin sheaths.
- Ninety percent of MS-related lesions can be detected on T2 MRI images.
- These lesions are typically para-ventricular, sometimes ovoid in shape (referred to as "Dawson's Fingers"), and often located on medullary veins.
- Calcium channel blockers, such as nicardipine, play an important role in treating arterial hypertension and cerebral vasospasm, both of which are associated with intracranial hematoma and increased intracranial hypertension.
- Many consider nicardipine to be an excellent choice for treating an acute hypertensive emergency in the setting of intracranial hemorrhage.
- Dosing should start at an infusion of 5 mg/hr. Titrate by 2.5 mg/hr every 5 to 15 minutes to desired effect, up to a maximum dose of 15 mg/hr.
Show References
Once you've punctured the spinal canal space during lumbar puncture, the following tips can be used to improve the rate of cerebrospinal fluid (CSF) flow, should it be suboptimal:
- Ask the patient to cough or bear down as in the Valsalva maneuver.
- Ask an assistant to intermittently press on patient's abdomen.
- Turn the spinal needle 90 degrees such that the bevel is cephalad.
- Use a larger diameter spinal needle (increases risk of post-lumbar puncture headache).
- Acute optic neuritis (ON) must be considered in any patient presenting with vision loss, especially if unilateral and associated with discomfort on eye movement.
- ON is a finding often (50%) associated with Multiple Sclerosis (MS), with or without other classic MS abnormalities such as transverse myelitis, internuclear ophthalmoplegia, and paresthesias.
- A normal fundoscopic examination does not rule out ON, as 50% of acute cases affect the retrobulbar space.
- Positive pertinent clinical findings may include an afferent pupillary defect in the affected eye and/or visual acuity abnormality, ranging from subtle deficit to total blindness.
Show References
- There are over 6 million stroke survivors in the United States, many of whom participate in helpful support groups, along with their loved ones and caregivers.
- Stroke recovery is often a lifelong journey.
- Prognosis and outcomes significantly improve with early, stroke rehabilitation at stroke-focused units.
- Stroke rehabilitation consists of several areas of focus such as physical, occupational, and visual therapies.
Stroke strikes F.A.S.T. and must be recognized quickly for optimized management.
The following Face, Arms, Speech test, known as F.A.S.T., is an easy and quick bedside teaching tool that can be used to spread awareness about how to recognize and respond to stroke symptoms:
F = Ask person to smile. Does one side of face droop down?
A = Ask person to raise both arms. Does one arm drift downward?
S = Ask person to say a simple phrase. Does speech sound slurred or strange?
T = If any of the above findings are observed, it's time to call 911 immediately.
Show References
- May is Stroke Awareness Month; Health care provider and patient education about how to prevent stroke is at least as important as treating it with cutting-edge therapies.
- Studies have shown that up to 80% of strokes could be prevented through recognition and management of risk factors, lifestyle changes, and compliance with recurrent stroke prevention treatments.
- Even in the emergency department, the opportunity to educate patients about the following stroke risk factors should be seized when possible:
-- Hypertension
-- Diabetes
-- Atrial Fibrillation
-- Hypercholesterolemia
-- Physical Inactivity
-- Tobacco Use
-- Alcohol Use
-- Obesity
Show References
- May is National Stroke Awareness Month. It is an important opportunity to foster education of the public and health care providers, which is a key component of stroke management. Awareness hastens recognition and optimized management.
- Clinicians can take part in public health initiatives by educating patients about the following signs and symptoms of acute stroke:
1. Walk; Is their balance off?
2. Talk; Is their speech slurred or face droopy?
3. Reach; Is one side weak or numb?
4. See; Is their vision all or partly lost?
5. Feel; Is their headache severe?
- This month, public education campaigns, through mechanisms such as billboard and mass transit advertisement, will be heightened, and can be used as additional tools for patient education.
- The terms pseudotumor cerebri, benign intracranial hypertension, and idiopathic intracranial hypertension (IIH), are all synonymous terms which describe a condition of elevated intracranial pressure (ICP), but the latter is the preferred term of use.
- IIH almost ubiquitously presents with a generalized headache and papilledema (i.e. fundoscopic examination imperative!). Visual disturbance and non-specific symptoms such as dizziness may also be present.
- Elevated ICP and papilledema are clinical emergencies until the presence or absence of an intracranial mass is confirmed.
- The following conditions must be met in order to diagnose IIH:
- Non-focal neurologic examination (except for 6th nerve palsy in some cases)
- Elevated opening pressure on lumbar puncture, > 20 to 25 mmH2O (perform only after risk for herniation assessed!)
- Normal cytologic and chemical cerebrospinal fluid analysis
- Small, symmetric brain ventricles on neuroimaging
- Exclusion of other sources of IH such as venous sinus thromboses by obtaining an MRI/venographic study of the head
Show References
- The Brachial Plexus is a bundle of nerve roots arising from C5, C6, C7, C8, and T1.
- Brachial plexus injuries (BPI) result from severe traction forces on the limb.
- The most common sources of BPI are motorcycle accidents and birth palsy (i.e. Erb or Duchenne Palsy) affecting the upper part of the plexus (C5, C6) and causing shoulder and biceps muscle weakness.
- Injury to C7 >>> wrist weakness.
- Injury to C8 and T1 >>> forearm and intrinsic hand muscle weakness.
- Injury to stellate ganglion or cervical sympathetic trunk >>> Horner's Syndrome.
- MRI of the upper extremity is the standard imaging modality used to make the diagnosis.