Search
121-140 of 543 results with category "Pediatrics"
Young infants (0-90 days) have immature immune systems and are at higher risk for serious bacterial infections, particularly urinary tract infections, bacterial meningitis, and bacteremia. Infants less than 90 days old have an incidence of bacterial infections between 8 to 12.5%, while infants less than or equal to 28 days old have almost a 20% incidence.
Risk-stratification of this group has been a huge focus of research over the past couple of decades to help identify which patients require a full sepsis work-up, particularly in well-appearing infants if a source of fever is identified early. Recent studies have explored the utility of biomarkers in risk stratification in this population. A better ability to discriminate would hopefully decrease unnecessary lumbar punctures, antibiotic use, and hospital admission. Multiple studies have shown procalcitonin is able to outperform CRP for prediction of serious bacterial infections. Kuppermann et al developed a tool to identify low risk febrile infants < 60 days using procalcitonin and ANC. Their prediction rule gave a 97.7% sensitivity, 60% specificity, and 99.6% NPV for serious bacterial infection. There have been several other studies that have looked harder to detect infections such as osteomyelitis or septic arthritis across all pediatric patients and the data has not been as promising.
Bottom line: Procalcitonin shows promise as part of a risk stratification tool in infants younger than 60 days. Other studies have failed to show its relevance as a screening tool for osteomyelitis, septic arthritis, renal abscess or community acquired pneumonia.
Show References
Several studies have described factors associated with peri-intubation cardiac arrest in the adult population. Factors such as pre-intubation hypotension, elevated BMI, and elevated shock index (HR/SBP) have been associated with cardiac arrest following intubation in adult ED patients. Given the differences in anatomy and physiology in children, one may expect risk factors for peri-intubation cardiac arrest to differ in children.
A number of studies have examined factors associated with peri-intubation cardiac arrest in the pediatric population, but these have remained limited to the inpatient setting. These studies have found that, in hospitalized and PICU patients, the factors of hemodynamic instability, hypoxemia, history of difficult airway, pre-existing cardiac disease, and higher number of intubation attempts are associated with peri-intubation cardiac arrest. A paucity of literature exists on this airway complication in pediatric ED patients.
Pokrajac et al. provide the first study on risk factors for peri-intubation cardiac arrest in pediatric ED patients. These authors conducted a retrospective nested case-control study of pediatric patients (ages <18 years) who presented to a tertiary children’s hospital in San Diego from 2009-2017. Cases included patients who had a cardiac arrest within 20 minutes after the start of endotracheal intubation. Authors selected a number of predictors to examine, including age-adjusted hemodynamic variables, capillary refill, pulse oximetry, patient characteristics, intubation-related factors, and pre-intubation interventions.
The authors found the following:
- Demographic characteristics:
o Patients with peri-intubation cardiac arrest were significantly younger (<1 year of age), shorter, and more likely to have history of preexisting pulmonary disease.
- Incident characteristics:
o Patients with peri-intubation cardiac arrest were more likely to have:
-Low or unobtainable SBP or DBP
-Delayed capillary refill time
-Low (<92%) or unobtainable pre-intubation SpO2
-More than 1 intubation attempt than controls
-No paralytic or sedative agent prior to intubation
o Patients with peri-intubation cardiac arrest were NOT more likely to have increases in age-adjusted HR or pediatric shock index in comparison to controls.
o The strongest clinical predictor for peri-intubation cardiac arrest was pre-intubation hypoxia or unobtainable SpO2. This fact is supported by children’s increased metabolic rate and thus increased oxygen consumption. This physiologic finding explains the shorter amount of time it takes children to develop acute hypoxia, particularly in the peri-intubation setting.
Bottom line: If planning to intubate a pediatric patient in the ED, keep in mind that pre-intubation systolic or diastolic hypotension, delayed capillary refill time, multiple intubation attempts, and hypoxia in particular may increase the risk for peri-intubation cardiac arrest. Consider providing apneic oxygenation to minimize hypoxemia prior to intubation.
Show References
To determine if the child is prepubescent, look for the lack of pubic hair, clitoral size, configuration of the hymen, breast development, and axillary hair growth. A Tanner stage of 1 would be consistent with prepuberty.
The proper positioning for the physical exam will allow the child to be comfortable and the examiner to obtain an adequate view including up to one-third of the vagina.
If the child is small enough, they can lay in the parent’s lap. For a larger child, you can have the parent sit in the bed with the patient or stand near the child’s head. Engage child life if available.
The frog leg position with gentle downward and outward traction of the labia at the 5- and 7-o’clock positions provides the optimal view.
The knee to chest position is helpful when further evaluation is needed.
A rectovaginal exam is useful for evaluation of masses or foreign body only and is not routinely needed. Place the examiner’s little finger in the rectum and the other hand on the abdomen and palpate.
The use of a vaginal speculum is rarely needed in prepubertal children; if it is needed, perform the exam under anesthesia.
Show References
Show References
The current COVID-19 pandemic and known aerosolized transmission has triggered many ED process changes, including the discouragement of utilizing nebulizers to administer inhaled bronchodilators such as albuterol for concern of spread. Historically, both patients and providers preferred the use of nebulizers as they are easier to use and the belief was that they were more effective than meterd dose inhalers. However, evidence based data has consistently shown that for both adult and pediatric patients that when MDI's are used WITH a spacer:
- There is NO significant difference in efficacy outcome.
- Nebs are associated with greater increase in tachycardia and tremors.
- Nebs are more costly overall.
- MDI's were associated with shorter ED stays and fewer hospital admissions for pediatric patients.
Albuterol: 2.5 mg nebulizer solution = 3-5 MDI puffs
Albuterol: 5 mg nebulizer solution = 5-10 MDI puffs
Ipratropium: 0.25 mg nebulizer solution = 2 MDI puffs
Ipratropium: 0.5 mg nebulizer solution = 4 MDI puffs
Show References
A labial adhesion is defined as a thin avascular clear plane, a raphe, between the labia minora. These adhesions which can be caused by minor trauma or infection in the absence of estrogen can cause varying degrees of obstruction.
Show References
Acute appendicitis is the most common etiology requiring urgent abdominal surgery in children in the United States. Peak incidence occurs in the second decade of life, with male patients being more commonly affected than female patients. Classic manifestations of appendicitis occur in school-aged children and adolescents, but are often absent in younger children. Infants and young children <5 years are more likely to present with nonspecific or atypical findings, resulting in delays in diagnosis and higher rates of perforation.
Diagnosis is aided by clinical factors, lab findings, and ultrasound (+/- CT or MRI if ultrasound is equivocal).
Historically, the standard of care for acute appendicitis has been urgent operative management. However, in the past several years, there has been increasing literature supporting nonoperative management (antibiotics only) in adult patients with acute uncomplicated appendicitis. Additionally, there is a growing body of evidence demonstrating the safety and efficacy of nonoperative management for uncomplicated appendicitis in children.
Hartford and Woodward provide a review of the current literature on the nonoperative management of uncomplicated appendicitis in children. They conclude:
- The majority of recent prospective studies demonstrate early treatment success (0-30 days) of approximately 90% in pediatric patients undergoing nonoperative management.
- Factors associated with failure of nonoperative management in pediatric appendicitis: longer duration of symptoms (>48 hours), younger age (<5 years), and presence of appendicolith.
- Nonoperative management has been associated with
o Lower healthcare costs at 1 year
o Fewer disability days at 1 year
o No significantly different rate of complicated appendicitis
- Most trials to date involve a 24-48 hour initial course of broad spectrum IV antibiotics followed by oral antibiotics for a total of >/= 7 days as nonoperative management. Currently, there is no consensus on antibiotic regimen.
Bottom Line: Given the current evidence, nonoperative management may be a viable treatment option for low risk pediatric patients with uncomplicated appendicitis. The literature is not conclusive, thus we as medical providers in conjunction with our surgical colleagues, should consider numerous factors when discussing treatment options for acute appendicitis with patients and their families.
Show References
- Urethral prolapse will appear as a protrusion of the distal urethra through the urinary meatus causing a “doughnut” sign.
- Risk factors include trauma, UTI, anatomical differences, and increased intraabdoiminal pressure from cough or constipation. There is a higher incidence in people of African descent.
- The chief complaint may include urethral mass and vaginal bleeding.
- There is a bimodal age distribution (prepuberty and postmetapause) due to a relative estrogen deficiency.
-Treatment is with estrogen cream and sitz baths for 4- 6 weeks.
Show References
Ingestion of a button battery is a can't-miss diagnosis with a very high risk for causing severe esophageal injury. There are about 3000 button battery ingestions per year, and this is increasing because electronics are becoming more and more prevalent.
Severe damage to the esophagus occurs within 2 hours. On your lateral view, the end with narrowing is the negative end, which triggers a hydrolysis reaction that results in an alkaline caustic injury and, ultimately, liquefactive necrosis.
Children can present with nonspecific symptoms and if the ingestion was not witnessed, they are at high risk for delays in diagnosis. Additionally, in the community setting, there can be further delays in definitive treatment (endoscopic removal) due to difficulty in calling teams in or transporting to other facilities.
Anfang et al. looked into ways to mitigate damage to esophageal tissue. They did an in vitro study on porcine esophageal tissue, measuring the pH with different substances applied. They tried apple juice, orange juice, gatorade, powerade, pure honey, pure maple syrup, and carafate. They then repeated the study in vivo on piglets with button batteries left in the esophagus and ultimately did gross and histological examination of the esophageal tissue.
Honey and carafate demonstrated protective effects both in vitro and in vivo. They neutralized pH changes, decreased full-thickness esophageal injury, and decreased outward extension of injury into deep muscle.
Take Home Point: If a child is found to have a button battery in the esophagus, while definitive management is still emergent endoscopic removal, early and frequent ingestion of honey (outside of the hospital) and Carafate (in the hospital) may help reduce the damage done to the tissue in the interim. The authors recommend 10ml every 10 minutes.
Show References
Definition: Congenital anomaly where the hymen is completely obstructing the vaginal opening
Demographic: Incidence 0.05-0.1% of females
History: Most are asymptomatic and diagnosed on physical exam or incidentally when there is lack of menarche. Symptoms in adolescents can include: Abdominal pain (50%), urinary retention (20%), abnormal menstruation (14%), dysuria (10%), frequency, renal failure, UTI and back pain.
Physical exam: bulging, blueish hymenal membrane
Complications: Late detection can lead to infections, fertility problems, endometriosis, hydronephrosis, and rarely renal failure
ED treatment: If abdominal pain is significant or there is urinary obstruction, a urinary foley can be placed. GYN should be consulted.
Definitive treatment: Hymenectomy, hymenotomy, carbon dioxide laser treatments or foley insertion through the hymen (done by a specialist).
Show References
There is no well validated clinical decision rule similar to NEXUS or the Canadian Cervical Spine rule in children for clearing the cervical spine. Clinical clearance versus imaging first is a complicated decision. Certain risk factors may predispose children to injury and should be taken into account when deciding about clinical clearance versus imaging (XR).
High Risk Criteria for Cervical Spine Injury in Pediatrics
| Mechanism
| High risk MVC Intrusion > 12 inches at the occupant site Intrusion > 18 inches at any site Partial or complete ejection Death in the same passenger compartment Vehicle telemetry consistent with high speed Fall > 10 feet Nonaccidental trauma Diving injury |
| History
| Down’s Syndrome 22.q11.2 deletion Klippel-Fiel syndrome |
| Physical Exam
| Altered mental status Intoxication Hypotension Focal neurological exam Neck pain Torticollis |
Show References
Every year, numerous children die of non-exertional heatstroke after being left in motor vehicles in the United States. Per data obtained from the national nonprofit KidsAndCars.org, the average number of pediatric vehicular heatstroke deaths is 39 per year since 1990. In 2018, this number peaked at 54 pediatric deaths. Prior studies show that the interior temperature of a closed vehicle rises quickly within minutes of closing the doors and windows. This rapid change occurs even on days with cooler ambient temperatures (20s °C/70s °F): the interior temperature of a car may still reach 117F within an hour.
Children, particularly infants and toddlers, are at increased risk for heat illness due to several physiologic and developmental factors:
- Unable to escape hot environments or to self-hydrate
- Lack mature thermoregulatory systems
o Have lower rate of sweat production than adults
- Have higher basal metabolic rates than adults
- Have higher body surface area:mass ratio --> absorb heat faster in hot environments
Bottom line: ED providers can be instrumental in giving anticipatory guidance on vehicular heatstroke in children during the warmer seasons:
- Educate caregivers to “Look before you Lock”
- Suggest that the caregiver place a valuable object (phone, employee badge, handbag) in the back seat when traveling with a child
- Remind caregiver of the dangers of intentionally leaving a child in the car for any reason, even during cooler spring/summer days.
Show Additional Information
Show References
Attachments
Show References
- Although significant data has been accumulated regarding Covid-19 infection in adults, the epidemiologic characters and clinical course descriptions in the pediatric population lags.
- Studies to date report that children have mild self-limiting disease with low mortality, even in Immunocompromised children.
- Less than half have fever.
- However, recent reports of a severe illness similar to Kawasaki Disease and/or toxic shock syndrome have led to the newly dubbed Multisystem Inflammatory Syndrome in Children (MIS-C)
- MIS-C CDC Criteria: <21 years of age, laboratory evidence of inflammation, clinically severe illness requiring hospitalization with multisystem involvement, no alternative diagnosis, and positive Covid-19 test or exposure within 4 weeks of presentation.
- MIS-C seems to spare infants and toddlers, and is mostly described in school aged and adolescent groups.
- MIS-C often begins with fever and GI symptoms (mild vague abdominal pain,diarrhea and/or vomiting).
- Telltale presentation of an erythematous rash that spares the limbs and is associated with conjunctival injection. Hence the initial misdiagnosis of Kawasaki and Toxic Shock in the first reported cases.
- MIS-C patients quickly decompensate to severe shock that is often refractory to typical treatments.
- Providers should have a higher index of suspicion for MIS-C in any child who presents with concern for Covid-19 infection with these symptoms, and especially with abnormal vital signs. Closer monitoring of heart rate and blood pressure, which is often neglected is vital.
Show References
NHTSA recommends that car seats be replaced following a moderate or severe crash. Car seats do not automatically need to be replaced following a minor crash.
A minor crash is one in which ALL of the following apply:
-The vehicle was able to be driven away from the crash site.
-The vehicle door nearest the car seat was not damaged.
-None of the passengers in the vehicle sustained any injuries in the crash.
-If the vehicle has air bags, the air bags did not deploy during the crash
-There is no visible damage to the car seat.
NEVER use a car seat that has been involved in a moderate to severe crash. Always follow manufacturer's instructions.
Show References
The leading cause of death in the US for those aged 16 to 24 years is motor vehicle collisions (MVCs). Teen drivers are more likely than any other age group to be involved in an MVC that result in injury or fatality. Texting while driving, nighttime driving, inexperienced driving, and driving under the influence of alcohol or drugs may play a role in these collisions.
Can anticipatory guidance related to safe driving be done in the ED? YES!
This study implemented a toolkit that contained a copy of the driving law, a sample parent-teen driving contract and statistics on teen driving injuries. Post toolkit questionnaires showed that both teens and their guardians learned new information.
Bottom line: Engage in anticipatory guidance in the ED with teens and their parents about seatbelt use, the dangers of driving under the influence and local driving laws.
Show References
Show References
Show References
Question
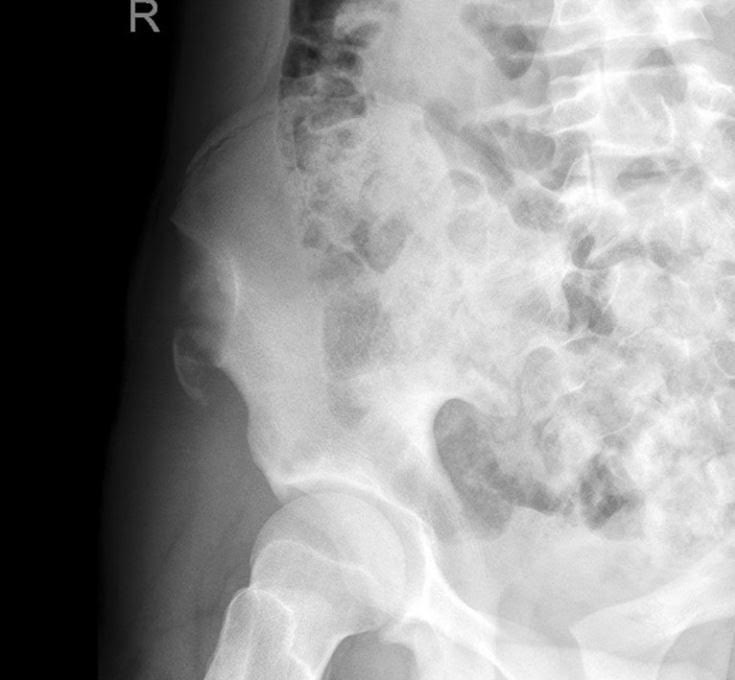
A 15 y.o. female presents to your emergency department with sudden onset hip pain after winding up to kick a soccer ball during her game today. You see a well-developed female in obvious discomfort, with tenderness to palpation over her lateral hip and pain with passive ROM at the hip. You obtain this x-ray. What is your diagnosis?
Show Answer
Show References
Tonsillectomy and adenoidectomy (T&A) is the second most common ambulatory surgery performed in the US. Children younger than 3 years, children with craniofacial disorders or sleep apnea are typically admitted overnight as studies have shown an increase rate of airway or respiratory complications in this population.
The most common late complications include bleeding and dehydration. Other complications include nausea, respiratory issues and pain.
Post-operatively, the overall 30-day emergency department return rate is up to 13.3%. Children ages 2 and younger were more likely to present to the ED. There is significantly higher risk of dehydration for children under 4 years. Children over the age of 6 had significantly higher bleeding risk and need for reoperation for hemorrhage control.