Search
261-280 of 860 results with category "Critical Care"
There are few conditions that can be as dramatic or difficult to control as variceal GI bleeding in a cirrhotic patient. It is important to be familiar with all options in these cases, from Blakemore/Minnesota tube placement to massive transfusion to when and which consultants to get involved. In cases that are refractory or not amenable to endoscopic intervention, emergent interventional radiology consultation for Transjugular Intrahepatic Portosystemic Shunt (TIPS) may be a consideration. In high risk cases, think about getting IR on the phone at the same time as you engage GI, in case endoscopic management fails. Variceal bleed patients can decompensate rapidly, get your consultants involved early!
Generally accepted indications for emergent TIPS (both of the following should be true):
-GI bleeding not amenable or not controllable by endoscopy
-Cause is felt to be variceal. May also consider in portal hypertensive gastropathy
Contraindications:
-Right heart failure or pulmonary hypertension
-Severe liver failure (MELD > 22, T Bili > 3 or Child-Pugh C. In these cases TIPS may not confer a significant survival benefit)
-Hepatic encephalopathy (relative contradindication. HE may be worsened by TIPS).
-Polycystic liver disease (makes TIPS technically challenging)
-Chronic portal vein thrombus (makes TIPS technically challenging. Acute PV thrombus is NOT considered a contraindication)
Bottom Line: In cases of variceal GI bleeding from portal hypertension, consider getting IR on the phone early to discuss emergent TIPS.
Show References
Pearl: consider desmopressin (DDAVP) for patients with an intracranial hemorrhage who are taking an antiplatelet. Caution, this is not for patients with an ischemic stroke with hemorrhagic conversion and it was not specifically evaluated for patients on anticoagulation or going to the OR with neurosurgery.
How strong is this evidence? International guidelines already give cautious approval for this practice, and now there is a retrospective review to support it. Though there were only 124 patients in the trial, the rate of hemorrhage expansion was much lower in the DDAVP group (10.9% vs 36.2%, P = .002) and there was no increased risk of hyponatremia (no events reported).
Show Additional Information
Show References
Interventions Shown to Reduce Mortality in RCTs
- Santacruz and colleagues recently performed a systematic review to determine which multicenter RCTs in critically ill patients have shown that an intervention was associated with a reduction in mortality.
- Approximately 13% of the 212 trials included in this review reported a statistically significant reduction in mortality. Unfortunately, many of the interventions were not associated with reduced mortality in subsequent studies.
- Interventions consistently shown to reduce mortality in multicenter RCTs in critically ill patients were limited tidal volume in patients with ARDS, noninvasive ventilation in acute hypercapnic respiratory failure, and noninvasive ventilation following extubation in complex cases.
- Corticosteroids in septic shock, selective digestive decontamination, and prone positioning in ARDS remain controversial.
Show References
Settings
- Patients: mechanical ventilation in the ICU. Randomization of 1000 patients.
- Intervention: conservative oxygen therapy, if spO2 reached 97%, then FiO2 was lowered to 0.21
- Comparison: no specific limits for FiO2 or SpO2.
- Outcome: number of ventilator-free days at 28 days after randomization.
Study Results:
- 484 conservative-oxygen group vs 481 to the usual oxygen group
- Comparing to the conservative-oxygen group had:
- more time at FiO2 21 (29 hours vs. 28 hours),
- less time with SpO2 > 97% (27 hours vs. 49 hours)
- Similar ventilator-free days: 21 days vs. 22 days.
Discussion:
This study’s results differed from previous single center study (Girardis JAMA 2016) or meta analysis (Chu DK, Lancer 2018), which showed mortality benefit in patients with conservative oxygen (Girardis & Chu) and more ventilator-free days (Girardis).
Conclusion: Conservative oxygen did not significantly affect the ventilator free days of mechanically ventilated patients.
Show References
When managing cardiac arrest, it is important to differentiate PEA, the presence of organized electrical activity without a pulse, from "pseudo-PEA,"where there is no pulse but there IS cardiac activity visualized on ultrasound.
Why:
- Pseudo-PEA is essentially a profound, low-flow shock state that often has reversible causes, such as hypovolemia, massive PE, tension pneumothorax, etcetera.
- Compared to PEA, with appropriate care patients with pseudo-PEA have a higher rate of ROSC as well as overall survival.
How:
- POCUS during rhythm check in cardiac arrest. Be careful not to prolong the pause in compressions; acquire the US, if needed, for review once hands are back on the chest.
What:
- In addition to searching for & addressing reversible causes of the pseudo-PEA, manage the profound shock state with pressors and/or inotropic support.
- In EDs where TEE is utilized during cardiac arrest resuscitations, strongly consider synchronization of external compressions with intrinsic cardiac activity to potentially improve ventricular filling and therefore coronary perfusion pressure.
Bottom Line: Pseudo-PEA is different from PEA. Utilize POCUS during your cardiac arrests to identify it and to help diagnose reversible causes, and treat it as a profound shock state with the appropriate supportive measures, i.e. pressors or inotropy.
Show References
Rapid Assessment of the RV on Bedside Echo
There are several causes of acute RV dysfunction resulting in a patient presenting to the ER with unstable hemodynamics. Some of these include acute cor pulmonale, acute right sided myocardial infarction and acute submassive or massive pulmonary embolism. While bedside assessment of the LV function is often performed by the ED physician, simultaneous evaluation of the RV can provide crucial information that can help guide therapeutic decisions to prevent worsening of the patient’s clinical condition. A rough guideline to determine RV size and function is below using the apical 4 chamber view.
Normal RV size : <2/3 the size of the LV
Mildly enlarged RV : >2/3 the size of the LV, but not equal in size
Moderately enlarged RV: RV size = LV size
Severely enlarged RV: RV size > LV size
Patients who are found to have RV dilation should be given fluids in a judicious fashion as the RV is not tolerant of fluid overload. Early diagnosis of the cause of acute RV failure should be sought to guide definitive therapy, but early institution of inotropic support should be considered. Frequent reassessments of biventricular function during resuscitation should be performed.
Show References
Attachments
Ever been in an acute rescucitation and found yourself unable to remember all of those famous ACLS Hs and Ts? I know I have. A few years ago Littman et al published an alternative approach to critically ill, hypotensive medical patients with non shockable rhythms. Unfortunately, it seems like some of the enthusiasm for this approach has died down, but I still think it's something you're more likely to recall in a pinch than the Hs and Ts and is a better way of getting started with a hypotensive non-trauma patient. And it's so simple you may actually remember it!
1) Look at the monitor. Is the rhythm narrow or wide?
2a) Narrow - more likely a mechanical problem (tamponade, tension PTX, autoPEEP, or PE). Give IVF and search for one of these causes (and correct it!). Keep in mind that ultrasound can help you differentiate a lot of these.
2b) Wide - more likely a metabolic problem (hyperK, sodium channel blockade, etc*). Give empiric calcium, bicarb, and other therapies targeted for these problems (if desired) and get stat labs.
Take a minute and either go to this REBEL EM post:
https://rebelem.com/a-new-pulseless-electrical-activity-algorithm/
To review this, or look at the attached diagrams.
*Dr. Mattu would want me to remind you that hyperkalemia IS a sodium channel poisoned state, so there's no need to think of these two separately
Show References
Attachments
- 1910292200_Narrow-Complex-PEA-Management-765x456.jpg (96 Kb)
- 1910292201_Wide-Complex-PEA-Management-765x444.jpg (83 Kb)
The Critically Ill Geriatric Patient with Sepsis
- Due to the age-related physiologic change of immunosenescence, geriatric patients have an increased susceptibility to infection, a decreased ability to mount a response to infection, and an increased likelihood of atypical presentations.
- Atypical presentations of sepsis in the geriatric patient include confusion, decreased functional status, generalized weakness, and failure to thrive.
- In fact, up to 33% of geriatric patients with bacteremia will be afebrile upon presentation.
- Consider sepsis in the differential diagnosis of geriatric patients with these nonspecific complaints.
Show References
Rationale: Data regarding temperature management in patients suffered from cardiac arrest with nonshockable rhythm was inconclusive.
Objective: whether moderate hypothermia at 33C, compared with normothermia at 37C would improve neurologic outcome in patients with coma after cardiac arrest with nonshockable rhythm.
Outcome: survival with favorable 90-day neurologic outcome (Cerebral Performance Category scale 1-2/5)
SummaryThere was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
This randomized multicenter trial involved 581 patients with cardiac arrest and nonshockable rhythm. Hypothermia group included 284 patients vs. 297 in the normothermia group. Median GCS at enrollment = 3.
Majority of patients was cooled with the use of a basic external cooling device: 37% for hypothermia and 50.8% for normothermia group.
There was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
Limitation:
A. The study used strict enrollment criteria:
- CPR initiation within 10 minutes;
- CPR to ROSC within 60 minutes;
- epinephrine or norepinephrine infusion at < 1 ug/kg/min;
- No Child-Pugh class C liver cirrhosis
B. normothermia group had higher proportion of patients with temperature at 38C.
C. Hypothermia group underwent temperature management of 56 hours vs. 48 hours for normothermia patients.
Take home points:
In a selected group of patients with cardiac arrest and nonshockable rhythm, moderate hypothermia at 33C may improve neurologic outcome.
Show References
Blood Transfusion Thresholds in Specific Populations
Sepsis - 7 g/dL
- non-inferior to 9 g/dL (which was previously recommended in early goal-directed therapy and early Surviving Sepsis guidelines)
Acute Coronary Syndrome - no current specific recommendations pending further studies
- recent MINT pilot study showed unexpected trend toward higher combined mortality and major cardiac events in restrictive transfusion arm (8 g/dL) vs. liberal arm (10 g/dL)
Stable Cardiovascular Disease - 8 g/dL
- no difference in 30-day mortality compared to 10 g/dL, excluding those who have undergone cardiac surgery
Gastrointestinal Bleeds
- UGIB - 7 g/dL (unless intravascularly volume depleted or h/o CAD)
- better 6 week-survival, less re-bleeding compared to 9 g/dL
- LGIB - 7 g/dL, limited evidence, but based on UGIB data
Acute Neurologic Injury - Traumatic Brain Injury - 7 g/dL
- no significant difference in neurologic recovery at 6 weeks or mortality vs. 10 g/dL, although there were more brain tissue hypoxia events in restrictive arm
- anemia and transfusions both associated with worse outcomes in TBI
Postpartum Hemorrhage - 1:1:1 ratio strategy
- FFP/RBC ratio ≥ 1 associated with improved patient outcomes
Show References
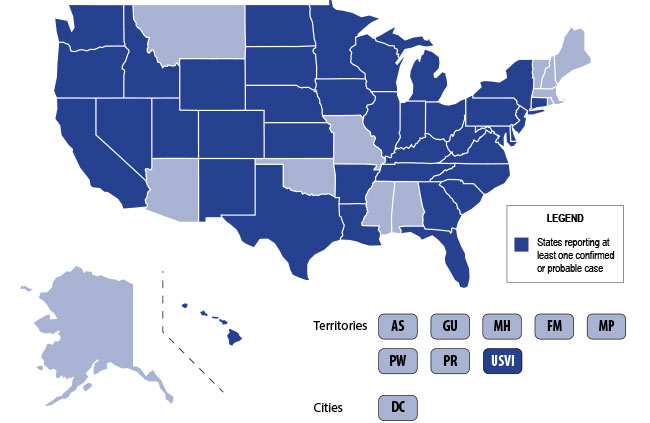
The U.S. is currently experiencing an epidemic of a severe lung disease termed Vaping-Associated Pulmonary Illness (VAPI), with over 500 cases and 7 deaths across 38 states and 1 U.S. territory since July 2019.
The clinical presentation of VAPI varies --
- Respiratory (SOB, cough, chest pain), constitutional (fever, tachycardia, headache, dizziness), and potentially GI symptoms (vomiting, diarrhea) after the use of vaping devices. GI symptoms may precede respiratory issues.
- Can take days or worsen over weeks and can present or end up with severe respiratory failure
Diagnostics --
- Labs nonspecific: Leukocytosis, elevated ESR, no specific infectious etiology
- Chest CT generally with bilateral infiltrates
- Bronchoscopy with BAL demonstrates PMNs and may have lipid-laden macrophages on Oil red O or Sudan staining
Treatment is supportive +/- steroids --
- Current recommendations to treat similarly to ARDS in intubated patients
- Potential benefit to steroids if not contraindicated
Bottom Line: Include vaping-associated pulmonary illness in your differential for patients presenting with acute lung disease.
- Ask patients about use of e-cigarette/vaping devices.
- Notify the CDC or your state health department of any suspected cases.
- Counsel your patients to avoid the use of these devices, at the very least until the specific causative agent is found.
Show Additional Information
Show References
Most non-OB physicians experience some fear or anxiety over taking care of the average pregnant patient. There are two patients to consider when caring for these women. Critical illness adds another layer of complexity to an already challenging patient population. Due to the normal physiologic changes that occur during pregnancy there are specific and important factors to be aware of when considering and preparing for intubation.
- Difficult intubations occur up to 5% of pregnant women.
- Edema occurs in the OP regions resulting in a narrowed OP diameter, especially with advancing gestational age. A smaller than anticipated ET tube might be necessary.
- Weight gain and/or obesity make visualization difficult Consider the ramp position to bring the external auditory meatus and the sternal notch into a horizontal line.
- Aortocaval compression decreases blood return to the heart and can result in hypotension on induction. Consider the use of a wedge under the patient’s right hip to decrease compression during intubation, especially those in later stages of pregnancy.
- Risk of aspiration is increased due to decreased lower esophageal sphincter tone. Consider administering metoclopramide prior to intubation which selectively increases esophageal sphincter.
- Functional residual volume in addition to increased oxygen consumption and metabolic demand lead to quicker desaturations and a greater intolerance to hypoxia and apnea.
- Be prepared with back up or adjunctive airway options including a video laryngoscope (like Glidescope), an LMA or a supraglottic airway. Although the LMA and supraglottic airways are rescue options in the setting of failed ET intubation, they can often adequately oxygenate and ventilate while urgently consulting with anesthesia colleagues in order to obtain a definitive airway.
Show References
It's important to remember the differential for the patient with Ventricular Assist Device (VAD) difficulties, as these patients are likely to show up in your ED.
1) Assess the patient as you usually would (signs of life, mental status, breathing, arrhythmias on monitor, etc). Listen for a hum over the chest. Don't expect to feel a pulse.
2) Look at the VAD including controller, driveline, and power source for alarms, disconnections, signs of infection, and other obvious issues.
3) Look at the power (displayed flow), pulsatility index, and pump speed on the controller to help determine the cause of the issue (see attached chart). Once you have a suspected etiology, typical management of these issues is usually similar to non-VAD patients (i.e. gentle IVF for hypovolemia, vasodilators if low flow is due to afterload/hypertension, defibrillation/CPR for arresting pts, etc).
Don't forget to call your VAD coordinator when able. Consider a-line placement for precise evaluation of blood pressure (focus on MAP).
Bottom Line: Consider obstruction/thrombosis, bleeding, infection, hypovolemia, afterload/hypertension, arrhythmia, worsening LV function, and suction events when troubleshooting VADs. The power, pulsatility index, and pump speed help differentiate these conditions.
Show References
Attachments
One third of your critically ill patients will have atrial fibrillation.
More than one third of those patients will develop immediate hypotension because of it.
More than one in ten will develop ischemia or heart failure because of it.
This is what you should know for your next shift:
#1 Don't wait to use electricity. If your patient is hypotensive or ischemic because of atrial fibrillation, you do not need to wait for anticoagulation before you cardiovert.
#2 Electricity buys you time to load meds. Fewer than half of patients you cardiovert will be in sinus rhythm an hour later and fewer than a quarter at the end of a day.
#3 There is no perfect rate control agent. Beta blockers have a lower mortality in A-fib from sepsis. Esmolol has the benefit of being short-acting if you cause hypotension. Diltiazem has better sustained control than amiodarone or digoxin.
#4 There is no perfect rhythm control agent. Magnesium is first-line in guidelines. Amiodarone can be used even when there is coronary artery or structural heart disease.
#5 Anticoagulation is controversial. In sepsis, anticoagulation does not reduce the rate of in-hospital stroke, but does increase the risk of bleeding. Use with caution if cardioversion isn't planned.
Show Additional Information
Show References
Critical Care Management of AIS
- In addition to reperfusion therapy, the critical care management of patients with an acute ischemic stroke also includes airway and ventilation management, hemodynamic management, glucose control, anticoagulation management, and surgery in select cases.
- Consider the following management pearls:
- Mechanical ventilation
- Target SpO2 > 94% (avoid supplemental oxygen for non-hypoxemic patients)
- Target normocarbia (PaCO2 35-45 mmHg)
- Hemodynamics
- Target euvolemia with isotonic saline
- Target BP < 185/110 mmHg for 24 hrs after tPA
- Target BP < 220/120 mmHg if tPA ineligible
- Target SBP < 160 mmHg after endovascular therapy
- Glucose
- Target serum glucose 140-180 mg/dL
- Mechanical ventilation
Show References
A new study confirmed the previously-known antibiotics to be associated with Torsades de pointes and QT prolongation (Macrolides, Linezolid, Imipenem and Fluoroquinolones). However, this study found new association between amikacin and Torsades de pointes/QT prolongation.
Methods
The authors queried the United States FDA Adverse Event Reporting System (FAERS) from 01/01/2015 to 12/31/2017 for reports of Torsade de points/QT prolongation (TdP/QT).
Reporting Odd Ratio (ROR) was calculated as the ratio of the odds of reporting TdP/QTP versus all other ADRs for a given drug, compared with these reporting odds for all other drugs present in FAERS
Results
FAERS contained 2,042,801 reports from January 1, 2015 to December 31, 2017. There were 3,960 TdP/QTP reports from the study period (0.19%).
Macrolides ROR 14 (95% CI 11.8-17.38)
Linezolid ROR 12 (95% CI 8.5-18)
Amikacin ROR 11.8 (5.57-24.97)
Imipenem-cilastatin ROR 6.6 (3.13-13.9)
Fluoroquinolones ROR 5.68 (95% CI 4.78-6.76)
Limitations:
These adverse events are voluntary reports
There might be other confounded by concomitant drugs such as ondansetron, azole anti-fungals, antipsychotics.
Show References
Torsades de pointes and QT prolongation Associated with Antibiotics
Methods
The authors queried the United States FDA Adverse Event Reporting System (FAERS) from 01/01/2015 to 12/31/2017 for reports of Torsade de points/QT prolongation (TdP/QT).
Reporting Odd Ratio (ROR) was calculated as the ratio of the odds of reporting TdP/QTP versus all other ADRs for a given drug, compared with these reporting odds for all other drugs present in FAERS
Results
FAERS contained 2,042,801 reports from January 1, 2015 to December 31, 2017. There were 3,960 TdP/QTP reports from the study period (0.19%).
Macrolides ROR 14 (95% CI 11.8-17.38)
Linezolid ROR 12 (95% CI 8.5-18)
Amikacin ROR 11.8 (5.57-24.97)
Imipenem-cilastatin ROR 6.6 (3.13-13.9)
Fluoroquinolones ROR 5.68 (95% CI 4.78-6.76)
Limitations:
These adverse events are voluntary reports
There might be other confounded by concomitant drugs such as ondansetron, azole anti-fungals, antipsychotics.
Bottom Line:
This study confimed the previously-known antibiotics to be associated with Torsades de pointes and QT prolongation (Macrolides, Linezolid, Imipenem and Fluoroquinolones). However, this study found new association between amikacin and Torsades de pointes/QT prolongation.
Show References
The Kidney Transplant Patient in Your ED
- Acute bacterial graft pyelonephritis is the most frequent type of sepis (bacterial pneumonia is the second most common source)
- Obtain renal transplant imaging to evaluate for sources of infection (i.e. urinary tract obstruction, renal abscess, or urine leakage)
- BK polyomavirus may reactivate and lead to nephritis, ureteral stenosis, or hemorrhagic cystitis
- Pneumocystis pneumonia is the most common fungal infection in patients without prophylaxis and after prophylaxis discontinuation (adjunctive steroids for treatment is controversial)
- Vascular access may be challenging. Avoid subclavian lines or femoral venous acess on the side of the graft
- Cardiovascular disease is the leading cause of mortality (accounts for 40-50% of deaths after the first year following renal transplant)
Show References
Managing the intubated patient with exacerbation of severe obstructive lung disease, especially asthma, can be very challenging as it carries higher risks of barotrauma due to higher pulmonary pressures and circulatory collapse due to auto-PEEP and decreased venous return. When measures such as medical therapy and noninvasive positive-pressure ventilation fail to prevent intubation, here are some tips to help:
1. Utilize a volume control ventilation mode to ensure a set tidal volume delivery / minute ventilation, as pressure-targeted modes will be more difficult due to the high pulmonary pressures in acute obstructive lung disease.
2. Set a low RR in order to allow for full exhalation, avoiding air-trapping / breath-stacking and circulatory collapse due to decreased venous return. This may require deep sedation and potentially paralysis.
- Permissive hypercapnea to >7.2 is generally well-tolerated except for pregnant patients, patients with high ICP, or patients with severe pulmonary hypertension
3. Increase your inspiratory flow by shortening your inspiratory time (thereby increasing your time for exhalation.
4. Monitor for auto-PEEP:
- Check your flow curve -- the waveform should return to zero before the start of the next inhalation, otherwise the next breath has been given before the patient has fully exhaled.
- Perform an expiratory hold at the end of exhalation. PEEP greater than set PEEP = auto-PEEP.
5. Peak inspiratory pressures will be high -- what is more important is the plateau pressure, measured by performing an inspiratory hold at the end of inspiration. Provided your plateau pressure remains <30, you don't need to worry as much about the peak pressure alarms.
6. If your patient acutely decompensates in terms of hemodynamics and oxygenation -- first attempt to decompress their likely auto-PEEPed lungs by popping them off the ventilator and manually press on their chest to assist with exhalation of stacked breaths allowing venous return to the heart.
Show References
With increasing critical care boarding and the opioid crisis leading to more intubations for overdose, extubation - which was once a very rare event in the ED - is taking place downstairs more often. Prolonged mechanical ventilation is associated with a ton of complications, so it's important for the ED physician to be comfortable assessing extubation readiness. There is no single accepted set of criteria, but most commonly used are some variant of the following:
- Reason for intubation (e.g. overdose, pneumonia, pulmonary edema, AMS, etc) has resolved
- Minimal vent settings - Typically FiO2 < 40%, PEEP <= 5
- Spontaneous breathing present (i.e. pt breathes with reasonable rate on PS, SIMV, VS, PPS, etc) and able to maintain reasonable pH and pCO2 on these settings
- Neuromuscular function adequate - Ask patient to lift head off bed
- Mental status adequate - Ask patient to give thumbs up or squeeze hands
- Secretions tolerable - Ask RN or RT for frequency of suctioning and sputum character. Think twice about extubation if getting purulent, thick secretions every 15 minutes.
- Clinical course does not require further intubation (i.e. no immediate trips planned to OR, MRI; pt not hemodynamically unstable, etc.)
If the above criteria are met, two additional tests are frequently considered:
- Spontaneous Breathing Trial (SBT) - Typically done by placing pt on PS with low settings (0/0 to 5/5). Let pt equilibrate (time of SBT is variable) on these settings, then calculate RSBI (RR/Vt). RSBI < 105 is traditionally considered acceptable for extubation. Remember - lower is better. Ask RT for this.
- Cuff Leak Test - becoming less popular, but may consider in patients at risk for laryngeal edema (e.g. prolonged intubation, angioedema, etc). Historically thought to predict airway swelling, but data is mixed. Ask RT for this.
And don't forget to consider extubating high risk patients directly to BiPAP or HFNC!
Bottom Line: For conditions requiring intubation where significant clinical improvement may be expected while in the ED (e.g. overdose, flash pulmonary edema, etc), be vigilant about, and have a system for, assessing readiness for extubation.