Search
341-346 of 346 results by Brian Corwell
Injury was originally described as an occupational hazard in Scottish gamekeepers (from breaking the necks of rabbits against the ground). Today, skiing is now the most common cause and injury is now the second most common orthopedic injury in skiers (MCL injury #1).
Injury to the ulnar collateral ligament (UCL) results from a sudden forced abduction (radial deviation) stress at the MCP joint of the thumb, commonly due to a fall against a ski pole or the ground.

http://blog.fitter1.com/wp-content/uploads/2010/04/b_14_1_2a.jpg
The most frequent site of rupture is the insertion into the proximal phalanx. The UCL may even avulse a small portion of the proximal phalanx at its insertion site.

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652013.jpg
Consider imaging before stress testing (to avoid further displacing a fracture)

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652060.jpg
Stabilize in a thumb spica splint and refer to hand surgery.
Calling this entity a “simple sprain” may result in chronic disability (chronic pain, instability, loss of pinch strength)
Show References
Supraspinatus: “Empty can” test. Have the patient abduct the shoulders to 90 degrees in forward flexion with the thumbs pointing downward. The patient attempts to lift the arms against the examiner’s resistance.
http://bjsportmed.com/content/42/8/628/F2.large.jpg
{kind=link}
Infraspinatus and teres minor: These muscles are responsible for external rotation of the shoulder. Have the patient flex both elbows to 90 degrees while the examiner provides resistance against external rotation.
http://www.physio-pedia.com/images/4/4b/Infraspinatus_test.jpg
{kind=link}
Subscapularis: “Lift-off” test. The patient rests the dorsum of the hand on the lower back (palm out) and then attempts to move the arm and hand off the back. Patients with tears may be unable to complete test due to pain.
http://www.aafp.org/afp/2008/0215/afp20080215p453-f4.jpg
{kind=link}
Show References
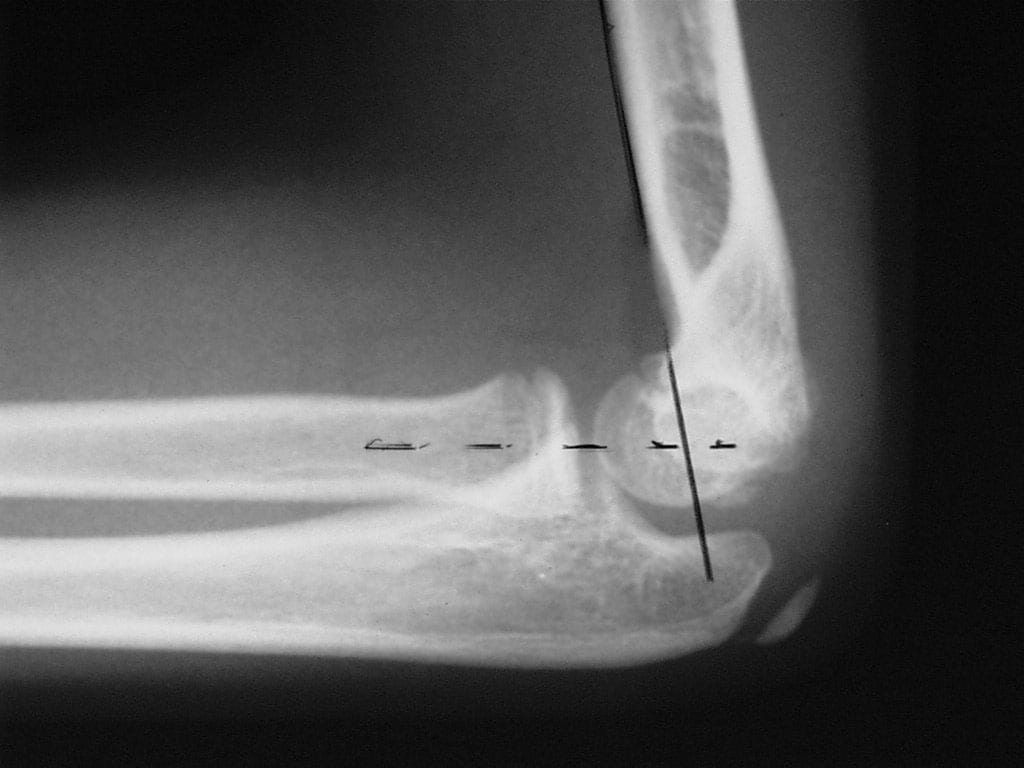
Radiologic evaluation of the elbow (Part 2)
Helpful clues in the evaluation of elbow trauma:
- The Anterior humeral line and the Radiocapitellar line
- The anterior humeral line: On a true lateral film, this line is drawn along the anterior aspect of the humeral shaft on the lateral radiograph This line passes through the middle one third of the capitellum in bones that are not injured. It is very useful for detecting subtle fractures.
- Fractures (i.e. supracondylar) usually result in displacement of the capitellum posteriorly.
- Thus, the anterior humeral line passes through the anterior one third or entirely anterior to the capitellum.
- The Radiocapitellar line: Since the radius articulates with the capitellum, a line is drawn through the middle of the radius shaft and extended proximally through the joint should bisect the capitellum on all views (AP & lateral).
- http://img.medscape.com/pi/emed/ckb/radiology/336139-415822-5412.jpg
- http://nypemergency.org/images/v2c18n.jpg
-
Improper alignment indicates a radial head dislocation (which may be very subtle)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Show References
Helpful clues in the evaluation of elbow trauma
Fat pads: The fat pad sign can be seen with any joint effusion (infection, inflammation) but in the setting of trauma, effusions are indicative of fractures about the elbow (even if no fracture line can be identified).
There are two fat pads within the elbow. Normally, on a true lateral radiograph only the anterior fat pad is seen as a small triangular radiolucent shadow anterior to the distal humeral diaphysis. The posterior fat pad is ordinarily not visualized on a lateral radiograph because it is tucked away within the olecranon fossa.
Normal lateral view: http://nypemergency.org/images/ElbowNormal.jpg
{kind=link}
With fractures, the joint becomes distended with blood. The anterior fat pad becomes displaced superiorly and outward from the humerus giving the so called "sail sign." Similarly, the posterior fat pad gets displaced out of the olecranon fossa and becomes visible on the lateral radiograph.
Anterior (sail) and posterior fat signs: http://nypemergency.org/images/Elbowsfatpadarrow.jpg
{kind=link}
Show References
- Back pain is the most common musculoskeletal complaint that results in visits to the ED.
- It has a benign course in more than 90% of patients, so we must be vigilant and comfortable looking for warning signs of a neurologically impairing or life-threatening cause.
- We rely on the presence of so-called "red flags" or alarm symptoms to guide further diagnostic tests, specialty evaluation, and treatment.
- Additionally, always consider 2 important extra-spinal causes of back pain: aortic dissection (sudden onset back pain) and abdominal aortic aneurysm (patients >50, esp. those who you think have a kidney stone- isolated back and groin pain is a common presentation).
| History and Physical Examination Red Flags | |
| Historical Red Flags | Physcial Red Flags |
| Age under 18 or over 50 Pain lasting more than 6 weeks History of cancer Fever and chills Night sweats, unexplained weight loss Recent bacterial infection Unremitting pain despite rest and analgesics Night pain Intravenous drug users, immunocompromised Major trauma Minor trauma in the elder | Fever Writhing in pain Bowel or bladder incontinence Saddle anesthesia Decreased or absent anal sphincter tone erianal or perineal sensory loss Severe or progressive neurologic defect Major motor weakness |
- Spondylolysis is a unilateral or bilateral defect in the pars interarticularis portion of the vertebrae.
- It is a stress fracture mostly seen in the lumbar vertebrae, and most commonly L5.
- Pain is relieved with rest and worsened by lateral bending or extension (NOTE: most back pain is worsened by flexion).
- If neurologic symptoms and/or radiculopathy are present, an alternative diagnosis should be considered, because they are rarely associated with spondylolysis.
- Diagnostic imaging should start with plain radiographs with added oblique views.
- Classically, oblique views show the Scotty dog sign with a crack on the dog’s neck/collar, the pars.
http://www.gentili.net/signs/images/400/spinescottyparsdefectdrawing.JPG
The Scotty dog’s head (superior articular facet), nose (transverse process), eye (pedicle), neck (pars interarticularis), and body (lamina) should be easily identified on the oblique radiograph.